

Red blood cell transfusion associated with increased morbidity and mortality in patients undergoing elective open abdominal aortic aneurysm repair
- PMID: 31295273
- PMCID: PMC6623955
- DOI: 10.1371/journal.pone.0219263
Red blood cell transfusion associated with increased morbidity and mortality in patients undergoing elective open abdominal aortic aneurysm repair
Abstract
Background: Red blood cell (RBC) transfusions are associated with increased mortality and morbidity. The aim of this analysis was to examine the association between RBC transfusions and long-term survival for patients undergoing elective open infrarenal abdominal aortic aneurysm (AAA) repair with up to 15 years of follow-up.
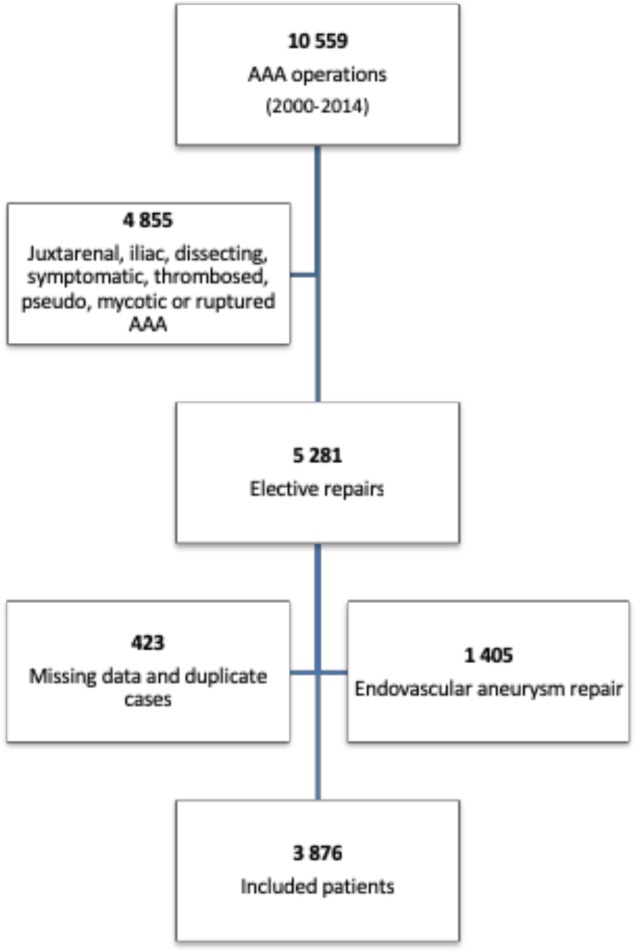
Methods: Prospective cohort study using data from The Danish Vascular Registry from 2000-2015. Primary endpoint was all-cause mortality. Secondary endpoints were in-hospital complications. Transfused patients were divided into subgroups based on received RBC transfusions (1, 2-3, 4-5 or > 5). Using Cox regression multi-adjusted analysis, non-transfused patients were compared to transfused patients (1, 2-3, 4-5, >5 transfusions) for both primary and secondary endpoints.
Results: There were 3 876 patients included with a mean survival of 9.1 years. There were 801 patients who did not receive transfusions. Overall 30-day mortality was 3.1% (121 patients) and 3.6% (112) for all transfused patients. For the five subgroups 30-day mortality was: No transfusions 1.1% (9 patients), 1 RBC 1.2% (4 patients), 2-3 RBC 2.2% (26 patients), 4-5 RBC 1.9% (14 patients) and > 5 RBC 7.9% (68 patients). After receiving RBCs, the hazard ratio for death was 1.54 (95% CI 1.27-1.85) compared to non-transfused patients. There was a significant increase in mortality when receiving 2-3 RBC: HR 1.32 (95% CI 1.07-1.62), 4-5 RBC: 1.64 (1.32-2.03) and >5 RBC: 1.96 (1.27-1.85) in a multi-adjusted model.
Conclusion: There is a dose-dependent association between RBC transfusions received during elective AAA repair and an increase in short- and long-term mortality. Approximately 25% of included patients had preoperative anemia. These findings should raise awareness regarding potentially unnecessary and harmful RBC transfusions.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



Similar articles
-
The effect of incremental increases in the number of packed red blood cell units transfused on perioperative outcomes in open abdominal aortic aneurysm repair.Vascular. 2025 Jun;33(3):504-510. doi: 10.1177/17085381241260925. Epub 2024 Jun 13. Vascular. 2025. PMID: 38872373
-
Changes in red blood cell transfusion practice during the turn of the millennium: a retrospective analysis of adult patients undergoing elective open abdominal aortic aneurysm repair using the Mayo database.Ann Vasc Surg. 2010 May;24(4):447-54. doi: 10.1016/j.avsg.2009.11.009. Epub 2010 Apr 2. Ann Vasc Surg. 2010. PMID: 20363103
-
Intraoperative use of packed red blood cell transfusion and mortality in patients undergoing abdominal or thoracoabdominal aortic aneurysm surgery.J Cardiovasc Surg (Torino). 2009 Aug;50(4):501-8. Epub 2009 Apr 1. J Cardiovasc Surg (Torino). 2009. PMID: 19339959
-
Massive Blood Transfusion in Patients with Ruptured Abdominal Aortic Aneurysm.Eur J Vasc Endovasc Surg. 2016 Nov;52(5):597-603. doi: 10.1016/j.ejvs.2016.07.023. Epub 2016 Sep 4. Eur J Vasc Endovasc Surg. 2016. PMID: 27605360
-
Open thoracic or thoracoabdominal aortic aneurysm repair after previous abdominal aortic aneurysm surgery.J Vasc Surg. 2008 Sep;48(3):761-8. doi: 10.1016/j.jvs.2008.02.006. Epub 2008 May 16. J Vasc Surg. 2008. PMID: 18486428 Review.
Cited by
-
Body mass index and mortality after elective open abdominal aortic aneurysm repair in a fifteen year multicenter cohort study.Sci Rep. 2025 Jun 3;15(1):19402. doi: 10.1038/s41598-025-05123-9. Sci Rep. 2025. PMID: 40461690 Free PMC article.
-
Prognostic value of extended cardiac risk assessment before elective open abdominal aortic surgery.Herz. 2024 Jun;49(3):210-218. doi: 10.1007/s00059-023-05209-y. Epub 2023 Oct 3. Herz. 2024. PMID: 37789149 English.
-
Tourniquet use for people with peripheral arterial disease undergoing major lower limb amputations.Cochrane Database Syst Rev. 2023 Jul 18;7(7):CD015232. doi: 10.1002/14651858.CD015232.pub2. Cochrane Database Syst Rev. 2023. PMID: 37462258 Free PMC article.
-
The Need for Red Cell Support During Non-Cardiac Surgery Is Associated to Pre-Transfusion Levels of FXIII and the Platelet Count.J Clin Med. 2020 Jul 31;9(8):2456. doi: 10.3390/jcm9082456. J Clin Med. 2020. PMID: 32751988 Free PMC article.
-
Risk factors of 30-day and long-term mortality and outcomes in open repair of thoracoabdominal aortic aneurysm.J Cardiothorac Surg. 2024 Apr 2;19(1):170. doi: 10.1186/s13019-024-02666-2. J Cardiothorac Surg. 2024. PMID: 38566230 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
