

Pre-operative stress testing in the evaluation of patients undergoing non-cardiac surgery: A systematic review and meta-analysis
- PMID: 31295274
- PMCID: PMC6622497
- DOI: 10.1371/journal.pone.0219145
Pre-operative stress testing in the evaluation of patients undergoing non-cardiac surgery: A systematic review and meta-analysis
Abstract
Background: Pre-operative stress testing is widely used to evaluate patients for non-cardiac surgeries. However, its value in predicting peri-operative mortality is uncertain. The objective of this study is to assess the type and quality of available evidence in a comprehensive and statistically rigorous evaluation regarding the effectiveness of pre-operative stress testing in reducing 30-day post -operative mortality following non -cardiac surgery.
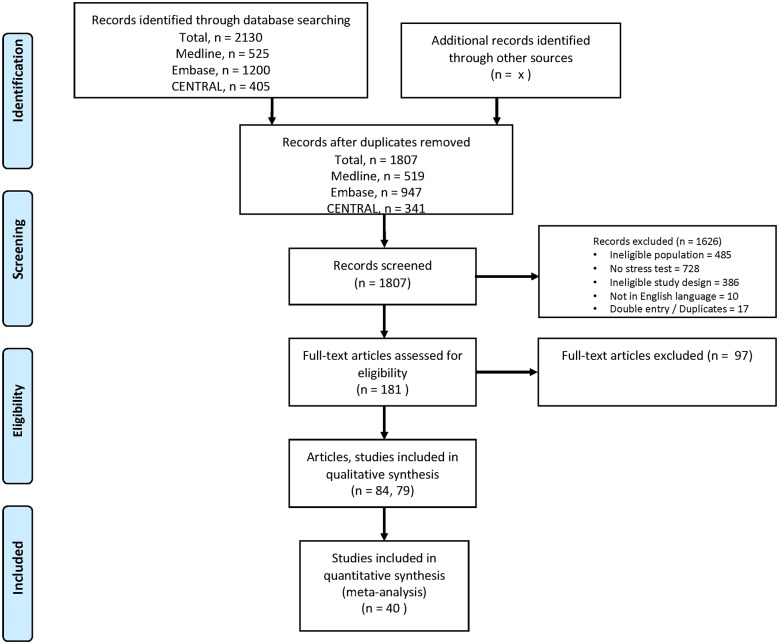
Methods: The databases of MEDLINE, EMBASE, and CENTRAL databases (from inception to January 27, 2016) were searched for all studies in English. We included studies with pre-operative stress testing prior to 10 different non-cardiac surgery among adults and excluded studies with sample size<15. The data on study characteristics, methodology and outcomes were extracted independently by two observers and checked by two other observers. The primary outcome was 30-day mortality. We performed random effects meta-analysis to estimate relative risk (RR) and 95% confidence intervals (95% CI) in two-group comparison and pooled the rates for stress test alone. Heterogeneity was assessed using I2 and methodological quality of studies using Newcastle-Ottawa Quality Assessment Scale. The predefined protocol was registered in PROSPERO #CRD42016049212.
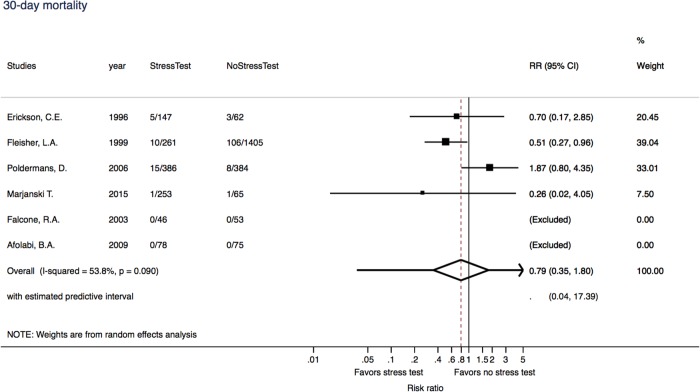
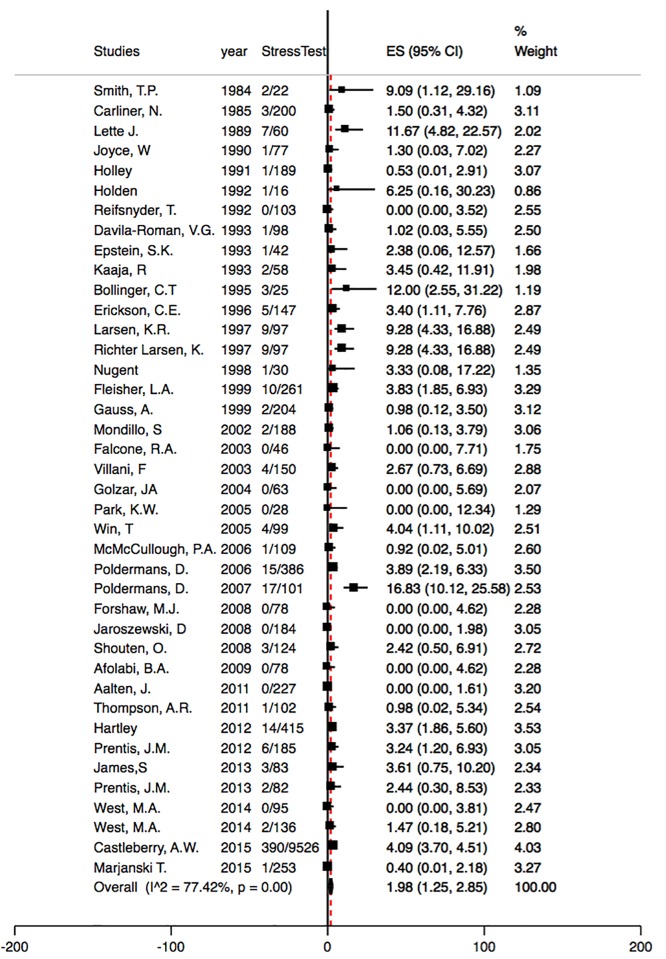
Results: From 1807 abstracts, 79 studies were eligible (297,534 patients): 40 had information on 30-day mortality, of which 6 studies compared stress test versus no stress test. The risk of 30-day mortality was not significant in the comparison of stress testing versus none (RR: 0.79, 95% CI = 0.35-1.80) along with weak evidence for heterogeneity. For the studies that evaluated stress testing without a comparison group, the pooled rates are 1.98% (95% CI = 1.25-2.85) with a high heterogeneity. There was evidence of potential publication bias and small study effects.
Conclusions: Despite substantial interest and research over the past 40 years to predict 30-day mortality risk among patients undergoing non-cardiac surgery, the current body of evidence is insufficient to derive a definitive conclusion as to whether stress testing leads to reduced peri-operative mortality.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Facility-level association of preoperative stress testing and postoperative adverse cardiac events.Heart. 2018 Dec;104(24):2018-2025. doi: 10.1136/heartjnl-2018-313047. Epub 2018 Jun 22. Heart. 2018. PMID: 29934371
-
The effects of perioperative β-blockers on mortality in patients undergoing non-cardiac surgery in real world: a meta-analysis of cohort studies.Int J Cardiol. 2014 Oct 20;176(3):605-10. doi: 10.1016/j.ijcard.2014.07.073. Epub 2014 Aug 4. Int J Cardiol. 2014. PMID: 25156833 Review.
-
Association between night/after-hours surgery and mortality: a systematic review and meta-analysis.Br J Anaesth. 2020 May;124(5):623-637. doi: 10.1016/j.bja.2020.01.019. Epub 2020 Mar 5. Br J Anaesth. 2020. PMID: 32147102
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
-
ß-Blockers reduce mortality in patients undergoing high-risk non-cardiac surgery.Am J Cardiovasc Drugs. 2010;10(4):247-59. doi: 10.2165/11539510-000000000-00000. Am J Cardiovasc Drugs. 2010. PMID: 20653331
Cited by
-
Association of metabolic equivalent of task (MET) score in length of stay in hospital following radical cystectomy with urinary diversion: a multi-institutional study.Int Urol Nephrol. 2021 Jul;53(7):1305-1310. doi: 10.1007/s11255-021-02813-x. Epub 2021 Mar 6. Int Urol Nephrol. 2021. PMID: 33675471 Free PMC article.
-
Growth Differentiation Factor 15: A Biomarker with High Clinical Potential in the Evaluation of Kidney Transplant Candidates.J Clin Med. 2020 Dec 20;9(12):4112. doi: 10.3390/jcm9124112. J Clin Med. 2020. PMID: 33419237 Free PMC article.
-
Clinical utility of preoperative stress perfusion cardiac magnetic resonance for predicting cardiovascular events in patients undergoing major noncardiac surgery.Ann Med. 2025 Dec;57(1):2489010. doi: 10.1080/07853890.2025.2489010. Epub 2025 Apr 7. Ann Med. 2025. PMID: 40193627 Free PMC article.
-
Preoperative Stress Testing before Non-Cardiac Surgery.Rev Cardiovasc Med. 2023 Mar 23;24(4):98. doi: 10.31083/j.rcm2404098. eCollection 2023 Apr. Rev Cardiovasc Med. 2023. PMID: 39076260 Free PMC article. Review.
-
NT-proBNP level as a substitute for myocardial perfusion scan in preoperative cardiovascular risk assessment in noncardiac surgery.BMC Anesthesiol. 2023 Jul 20;23(1):244. doi: 10.1186/s12871-023-02205-x. BMC Anesthesiol. 2023. PMID: 37474913 Free PMC article.
References
-
- Kristensen SD, Knuuti J, Saraste A, Anker S, Botker HE, Hert SD, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J. 2014;35(35):2383–431. Epub 2014/08/03. 10.1093/eurheartj/ehu282 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
