

Delayed lupus nephritis in the course of systemic lupus erythematosus is associated with a poorer treatment response: a multicentre, retrospective cohort study in Japan
- PMID: 31296139
- PMCID: PMC6681441
- DOI: 10.1177/0961203319860200
Delayed lupus nephritis in the course of systemic lupus erythematosus is associated with a poorer treatment response: a multicentre, retrospective cohort study in Japan
Erratum in
-
Corrigendum to delayed lupus nephritis in the course of systemic lupus erythematosus is associated with a poorer treatment response: a multicentre, retrospective cohort study in Japan.Lupus. 2019 Oct;28(11):1383. doi: 10.1177/0961203319869574. Epub 2019 Aug 23. Lupus. 2019. PMID: 31441372 Free PMC article. No abstract available.
Abstract
Objective: The objective of this study was to investigate possible differences in treatment responses between two categories for the onset of lupus nephritis.
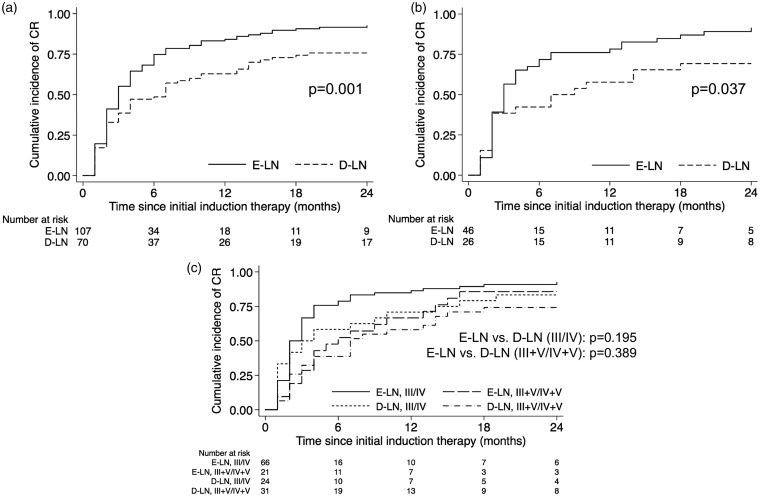
Methods: We performed a multicentre, retrospective cohort study of class III-V lupus nephritis patients diagnosed between 1997 and 2014. The renal responses to initial induction therapy were compared between patients who developed lupus nephritis within one year from diagnosis of systemic lupus erythematosus (early (E-) LN) and the remainder (delayed (D-) LN) using the Kaplan-Meier method. We determined the predictors of renal response as well as renal flares and long-term renal outcomes using multivariate Cox regression analyses.
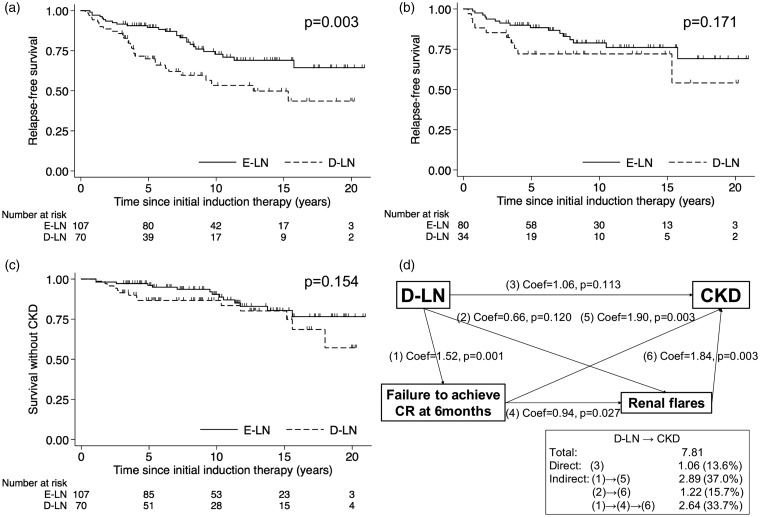
Results: A total of 107 E-LN and 70 D-LN patients were followed up for a median of 10.2 years. Log-rank tests showed a lower cumulative incidence of complete response in D-LN compared with E-LN patients. Multivariate analysis identified D-LN (hazard ratio (HR) 0.48, 95% confidence interval (CI) 0.33-0.70), nephrotic syndrome at baseline, and a chronicity index greater than 2 as negative predictors of complete response. D-LN patients were more likely to experience renal flares. D-LN (HR 2.54, 95% CI 1.10-5.83) and decreased renal function were significant predictors of chronic kidney disease at baseline.
Conclusion: D-LN was a predictor of poorer treatment outcomes, in addition to renal histology and severity of nephritis at lupus nephritis onset.
Keywords: Lupus nephritis; delayed lupus nephritis; systemic lupus erythematosus; treatment response.
Figures
Similar articles
-
Lupus nephritis among 624 cases of systemic lupus erythematosus in Riyadh, Saudi Arabia.Rheumatol Int. 2009 Jul;29(9):1057-67. doi: 10.1007/s00296-009-0905-8. Epub 2009 Apr 21. Rheumatol Int. 2009. PMID: 19381639
-
Chronicity index, especially glomerular sclerosis, is the most powerful predictor of renal response following immunosuppressive treatment in patients with lupus nephritis.Int J Rheum Dis. 2018 Feb;21(2):458-467. doi: 10.1111/1756-185X.13254. Epub 2018 Jan 5. Int J Rheum Dis. 2018. PMID: 29314776
-
Combination immunosuppressant therapy and lupus nephritis outcome: a hospital-based study.Lupus. 2019 Apr;28(5):658-666. doi: 10.1177/0961203319842663. Epub 2019 Apr 10. Lupus. 2019. PMID: 30971165
-
Lupus Nephritis: A Treatment Update.Curr Clin Pharmacol. 2018;13(1):4-13. doi: 10.2174/1574884713666180403150359. Curr Clin Pharmacol. 2018. PMID: 29611488 Review.
-
Pediatric lupus nephritis: more options, more chances?Lupus. 2013 May;22(6):545-53. doi: 10.1177/0961203313485490. Epub 2013 Apr 29. Lupus. 2013. PMID: 23629826 Review.
Cited by
-
Treatment outcome and survival status among adult patients treated for lupus nephritis in selected tertiary hospitals of Ethiopia.Sci Rep. 2024 Mar 7;14(1):5603. doi: 10.1038/s41598-024-56317-6. Sci Rep. 2024. PMID: 38454130 Free PMC article.
-
Comparison of complete renal response and mortality in early- and late-onset lupus nephritis: a multicenter retrospective study of a Japanese cohort.Arthritis Res Ther. 2020 Jul 22;22(1):175. doi: 10.1186/s13075-020-02271-3. Arthritis Res Ther. 2020. PMID: 32698892 Free PMC article.
-
Risk factors for subsequent lupus nephritis in patients with juvenile-onset systemic lupus erythematosus: a retrospective cohort study.Pediatr Rheumatol Online J. 2023 Mar 24;21(1):28. doi: 10.1186/s12969-023-00806-x. Pediatr Rheumatol Online J. 2023. PMID: 36964531 Free PMC article.
-
Clinical and laboratory characteristics of early-onset and delayed-onset lupus nephritis patients: A single-center retrospective study.Rheumatol Int. 2024 Jul;44(7):1283-1294. doi: 10.1007/s00296-024-05579-4. Epub 2024 Mar 28. Rheumatol Int. 2024. PMID: 38546745 Free PMC article.
-
Worse Renal Presentation and Prognosis in Initial-Onset Lupus Nephritis than Early-Onset Lupus Nephritis.Yonsei Med J. 2020 Nov;61(11):951-957. doi: 10.3349/ymj.2020.61.11.951. Yonsei Med J. 2020. PMID: 33107238 Free PMC article.
References
-
- Cervera R, Khamashta MA, Font J, et al. Morbidity and mortality in systemic lupus erythematosus during a 10-year period: a comparison of early and late manifestations in a cohort of 1,000 patients. Medicine (Baltimore) 2003; 82: 299–308. - PubMed
-
- Faurschou M, Dreyer L, Kamper AL, Starklint H, Jacobsen S. Long-term mortality and renal outcome in a cohort of 100 patients with lupus nephritis. Arthritis Care Res 2010; 62: 873–880. - PubMed
-
- Illei GG, Takada K, Parkin D, et al. Renal flares are common in patients with severe proliferative lupus nephritis treated with pulse immunosuppressive therapy: long-term followup of a cohort of 145 patients participating in randomized controlled studies. Arthritis Rheum 2002; 46: 995–1002. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
