

Evaluation of 30-Day Hospital Readmission and Mortality Rates Using Regression-Discontinuity Framework
- PMID: 31296295
- PMCID: PMC8669780
- DOI: 10.1016/j.jacc.2019.04.060
Evaluation of 30-Day Hospital Readmission and Mortality Rates Using Regression-Discontinuity Framework
Abstract
Background: The Hospital Readmissions Reduction Program (HRRP) has been associated with reduced 30-day readmissions for acute myocardial infarction (AMI) and heart failure (HF).
Objectives: The purpose of this study was to test whether this 30-day readmission reduction is a manifestation of practices that defer or avoid hospitalizations beyond the 30-day period.
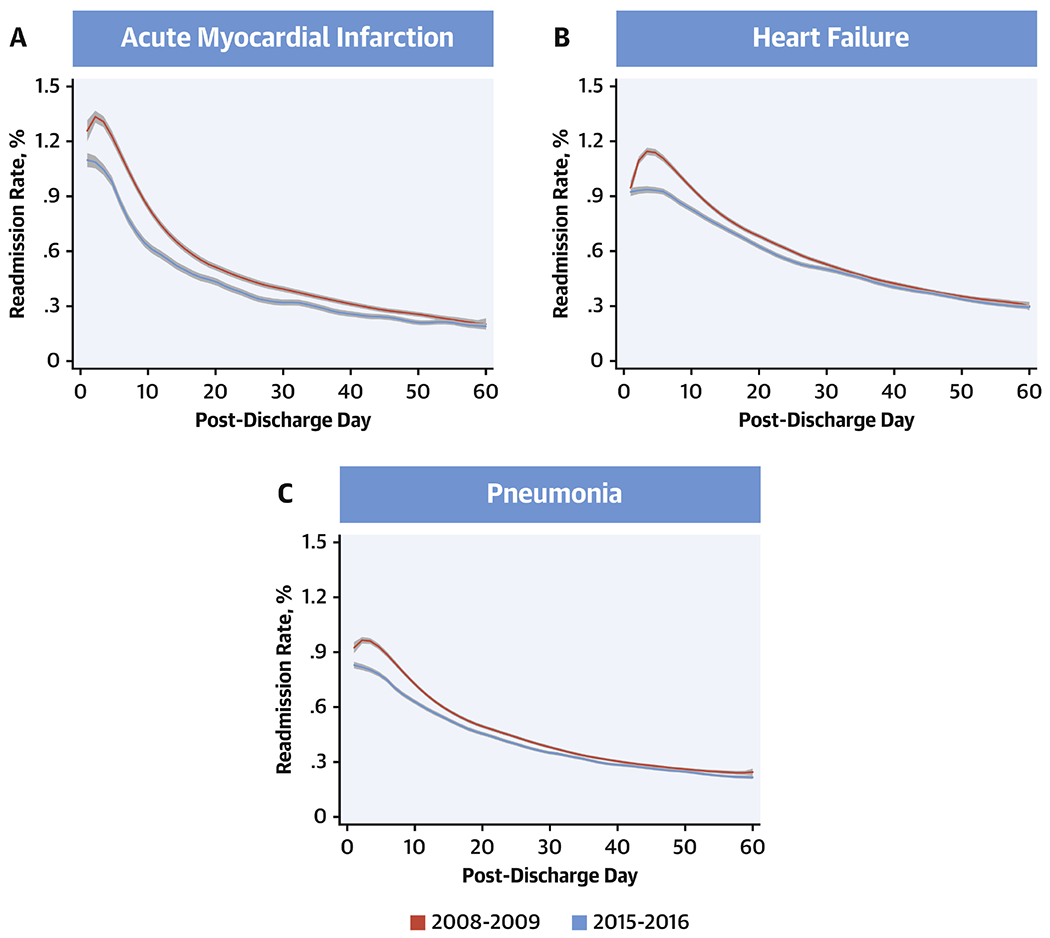
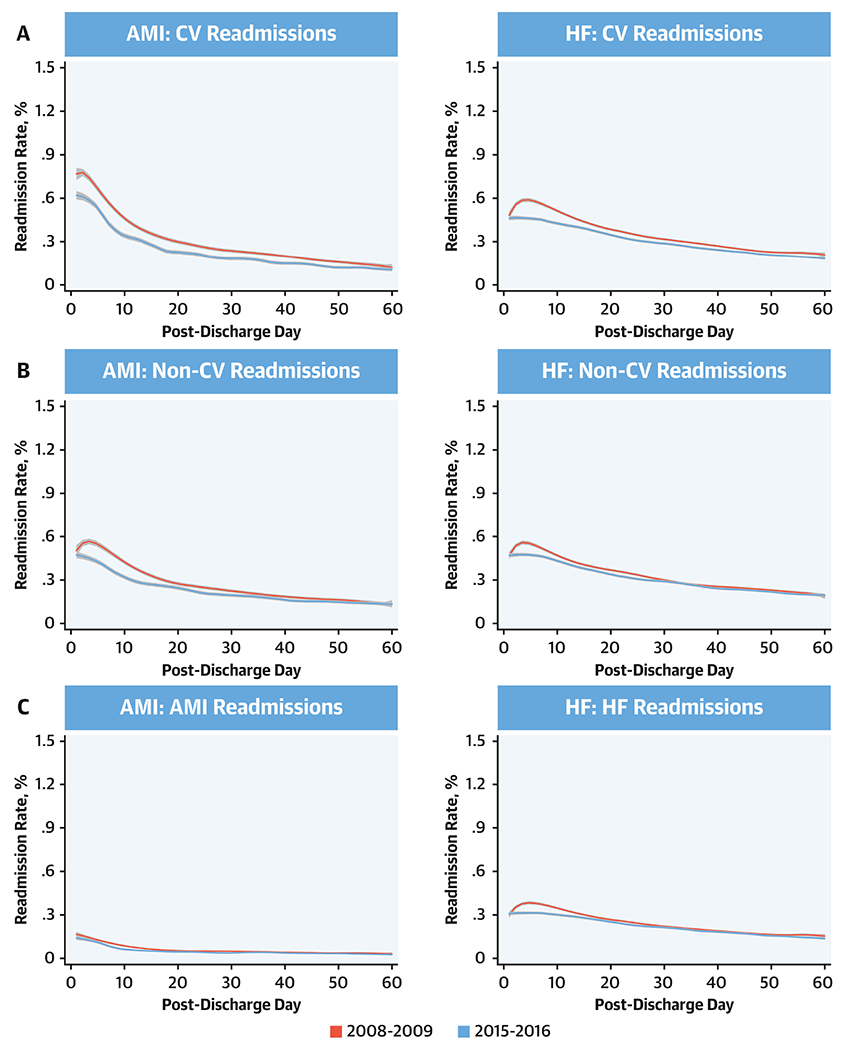
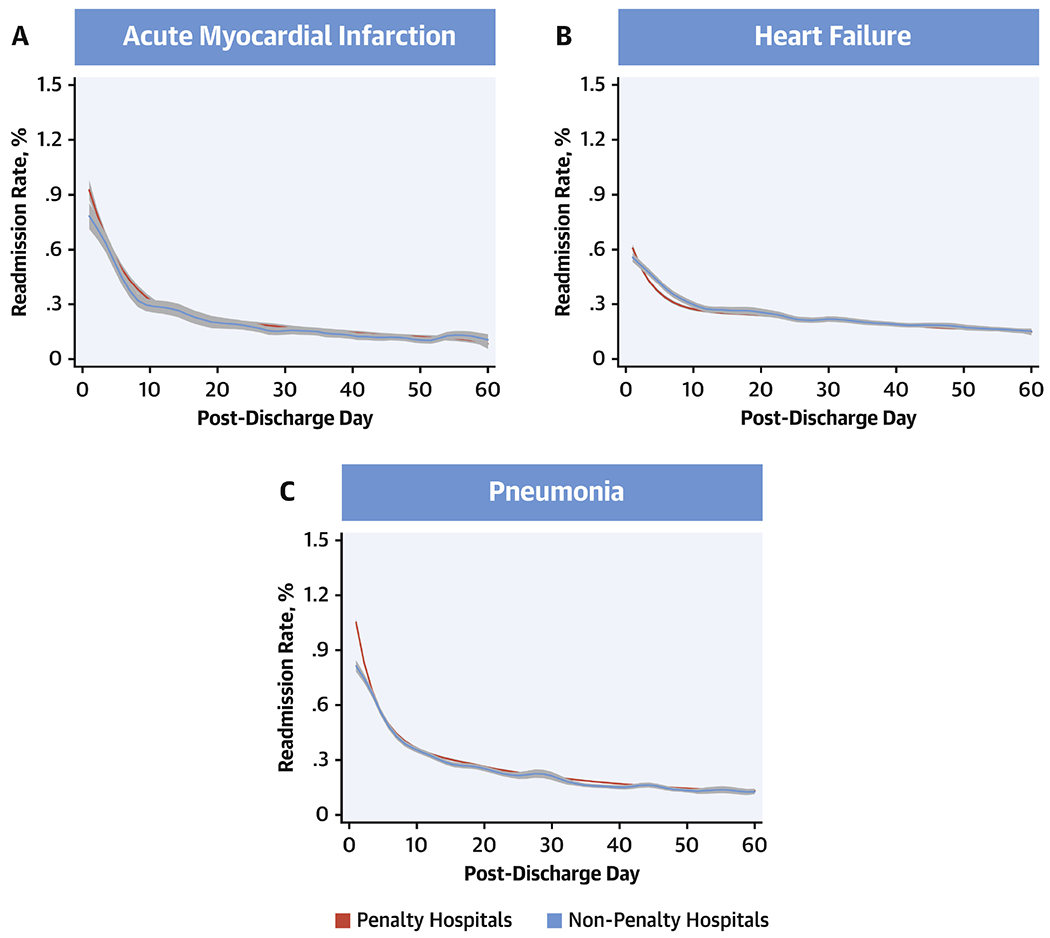
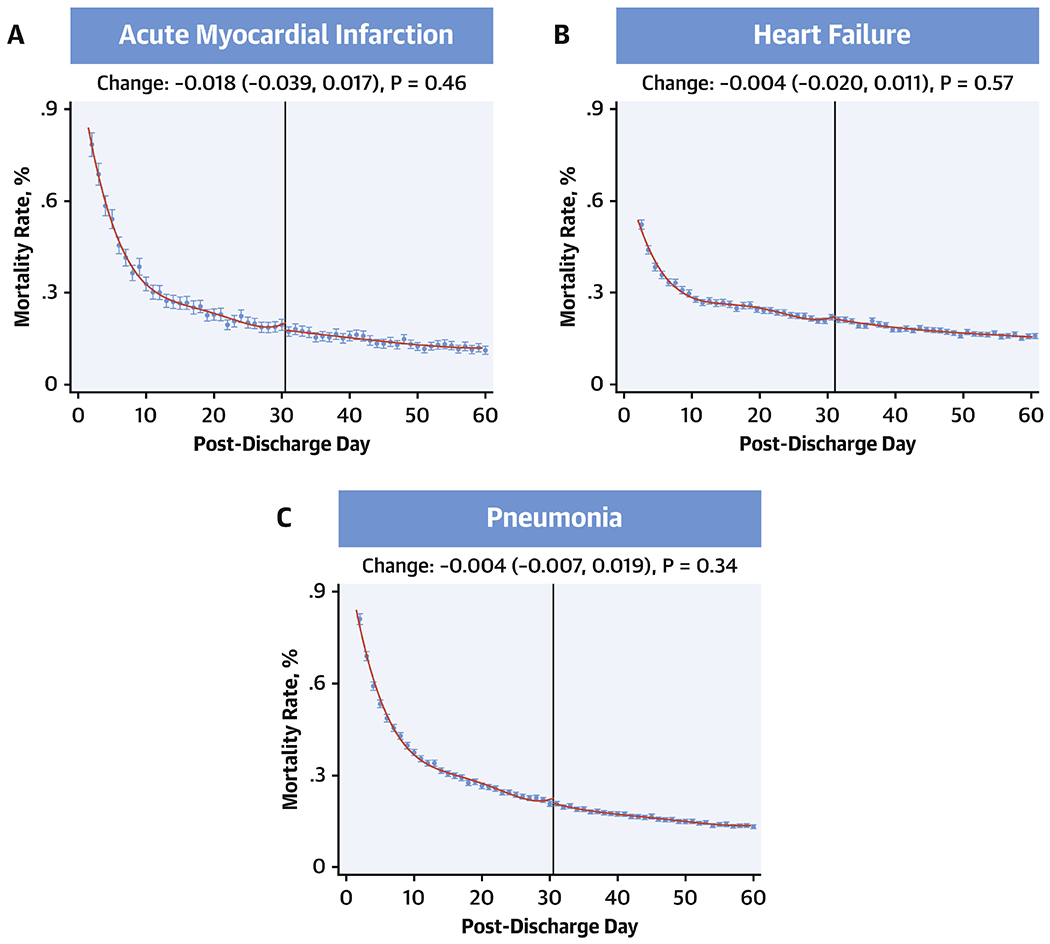
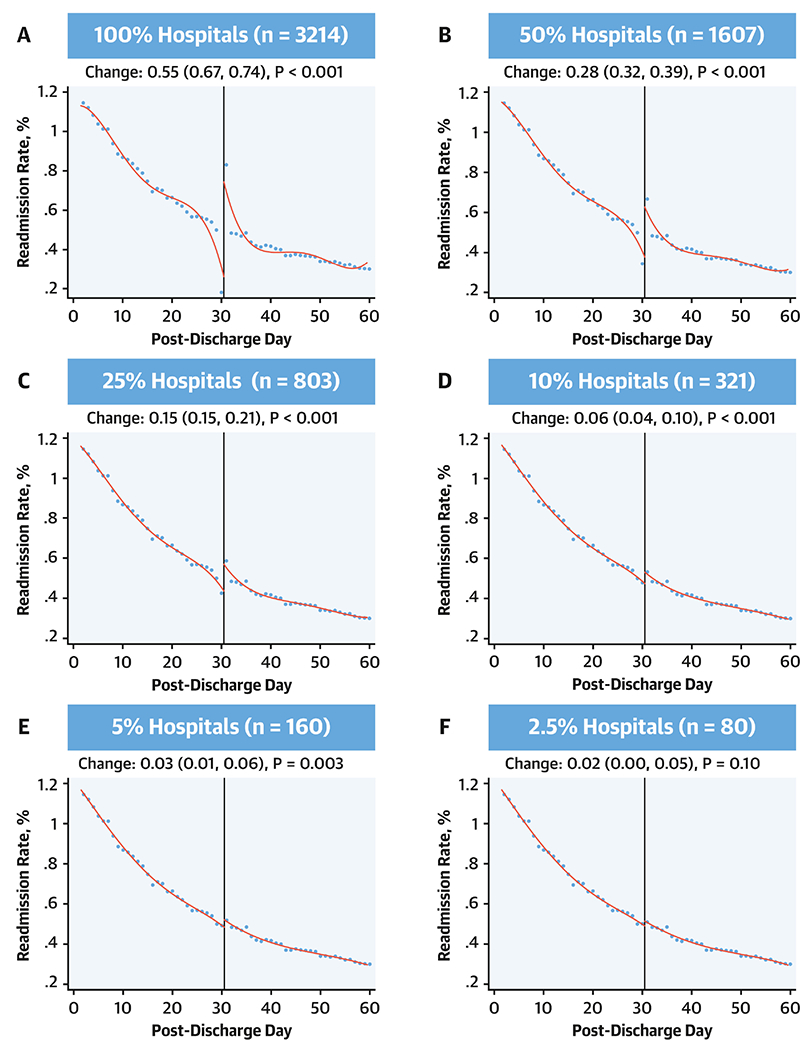
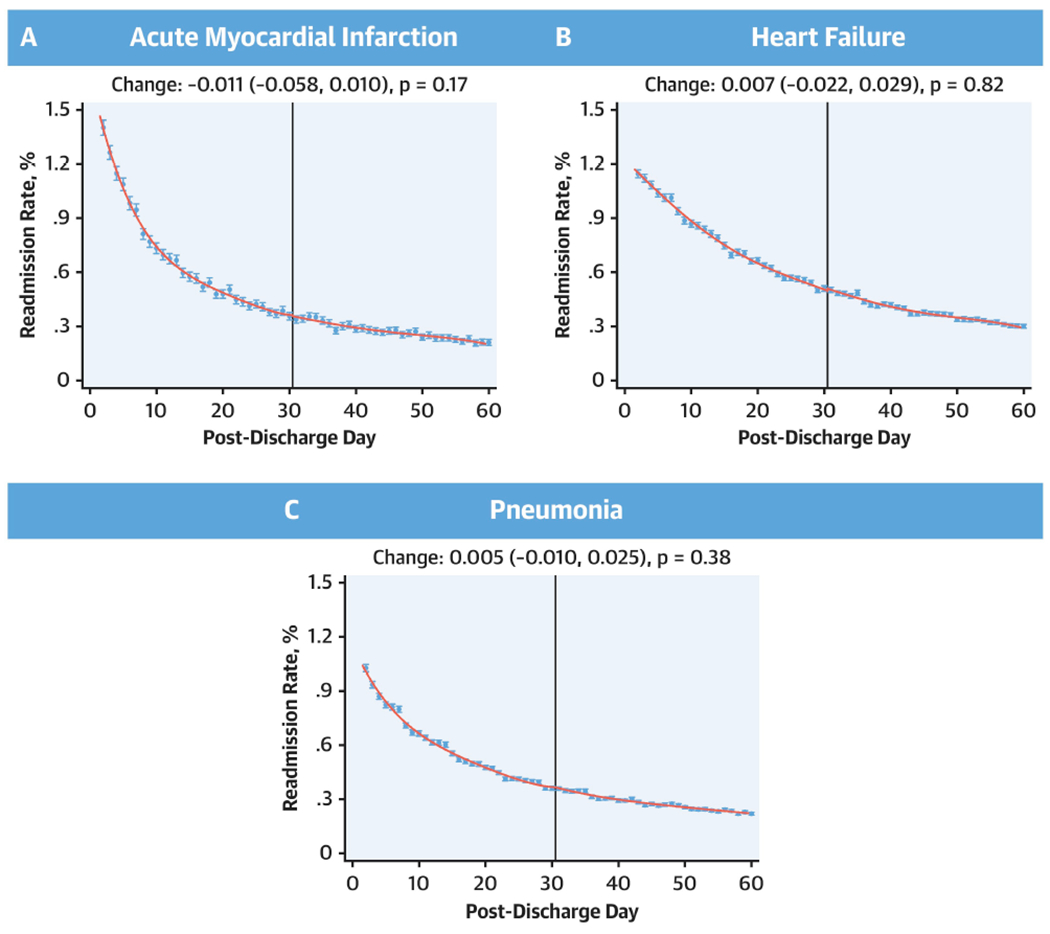
Methods: At all U.S. hospitals under HRRP, the authors calculated daily readmission rates for elderly Medicare fee-for-service beneficiaries through day-60 post-discharge following a hospitalization for AMI and HF-the 2 target cardiovascular conditions-as well as pneumonia in July 2008 to June 2016. The authors applied a robust bias-corrected nonparametric regression approach to evaluate for discontinuities in rates around day 30.
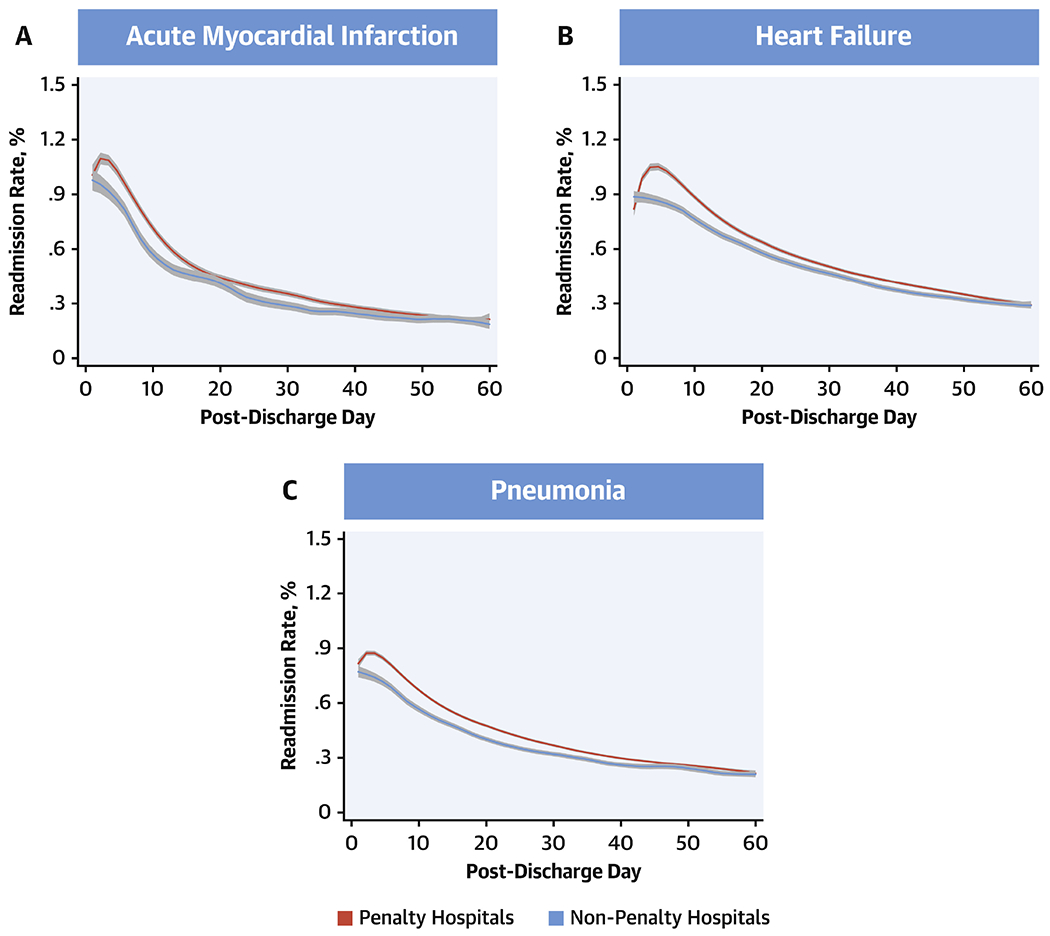
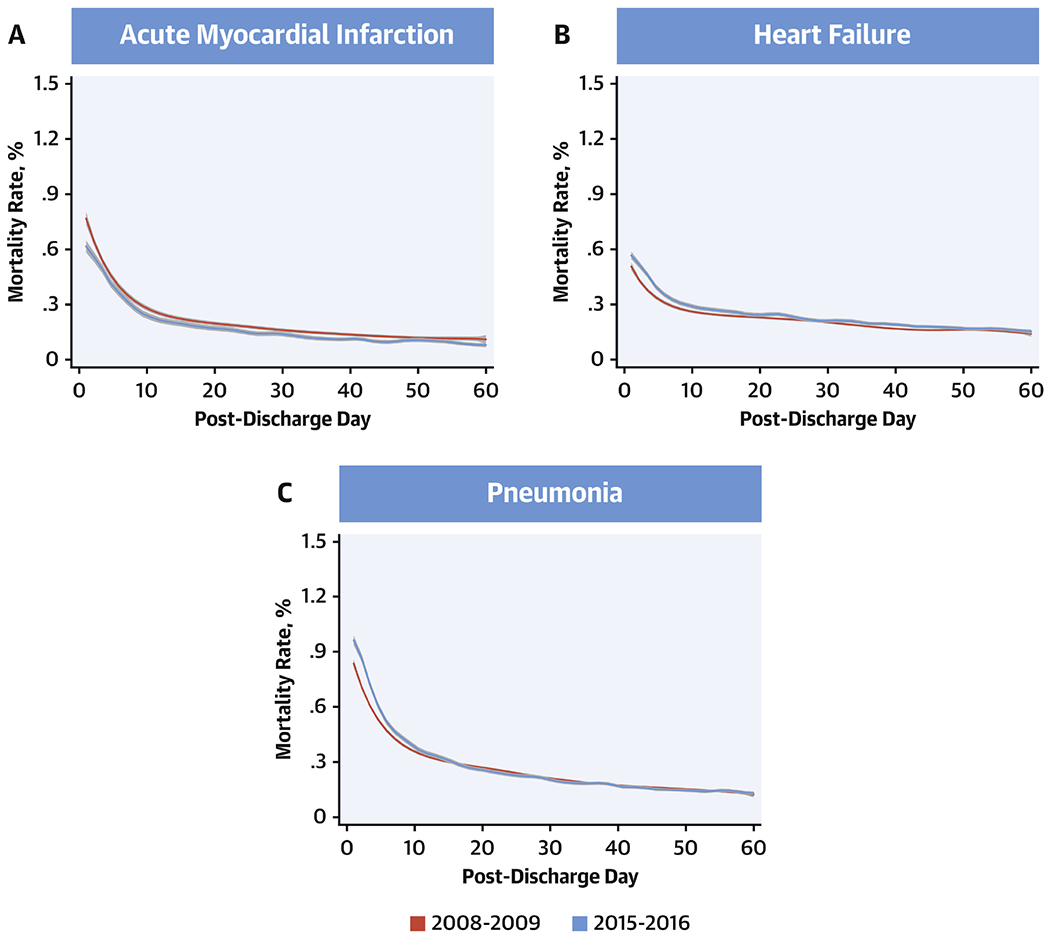
Results: The authors identified 3,256 eligible hospitals, with median readmission rates in the days 1 to 30 and 31 to 60 post-discharge of 19.6% (interquartile range [IQR]: 16.7% to 22.9%) and 7.8% (IQR: 6.5% to 9.4%) for AMI, 23.0% (IQR: 20.6% to 25.3%) and 11.4% (IQR: 10.2% to 12.6%) for HF, and 17.5% (IQR: 15.4% to 19.8%) and 8.3% (IQR: 7.3% to 9.3%) for pneumonia, respectively. Daily readmission rates decreased across most of the 60 post-discharge days, with no discontinuities in the local polynomial regression for readmission at the 30-day mark, with a >95% power to detect 0.1% difference for each outcome across post-discharge day 30. Similarly, there was no discontinuity in mortality at 30 days post-discharge, or for either outcome at hospitals that incurred readmission penalties.
Conclusions: There was no evidence that clinicians adopted strategies that specifically deferred admissions or affected mortality in the 30-day period after discharge. The findings are consistent with the institution of strategies that generally affected readmission risk after discharge.
Keywords: Hospital Readmissions Reduction Program; health policy; outcomes research; quality of care.
Copyright © 2019 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Evolving the Hospital Readmissions Reduction Program: A Call for Peace, Happiness, and Improved Patient-Centered Outcomes.J Am Coll Cardiol. 2019 Jul 16;74(2):235-237. doi: 10.1016/j.jacc.2019.05.030. J Am Coll Cardiol. 2019. PMID: 31296296 No abstract available.
References
-
- Zuckerman RB, Sheingold SH, Orav EJ, Ruhter J, Epstein AM. Readmissions, observation, and the Hospital Readmissions Reduction Program. N Engl J Med 2016;374:1543–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
