

Cardiac MRI Endpoints in Myocardial Infarction Experimental and Clinical Trials: JACC Scientific Expert Panel
- PMID: 31296297
- PMCID: PMC7363031
- DOI: 10.1016/j.jacc.2019.05.024
Cardiac MRI Endpoints in Myocardial Infarction Experimental and Clinical Trials: JACC Scientific Expert Panel
Abstract
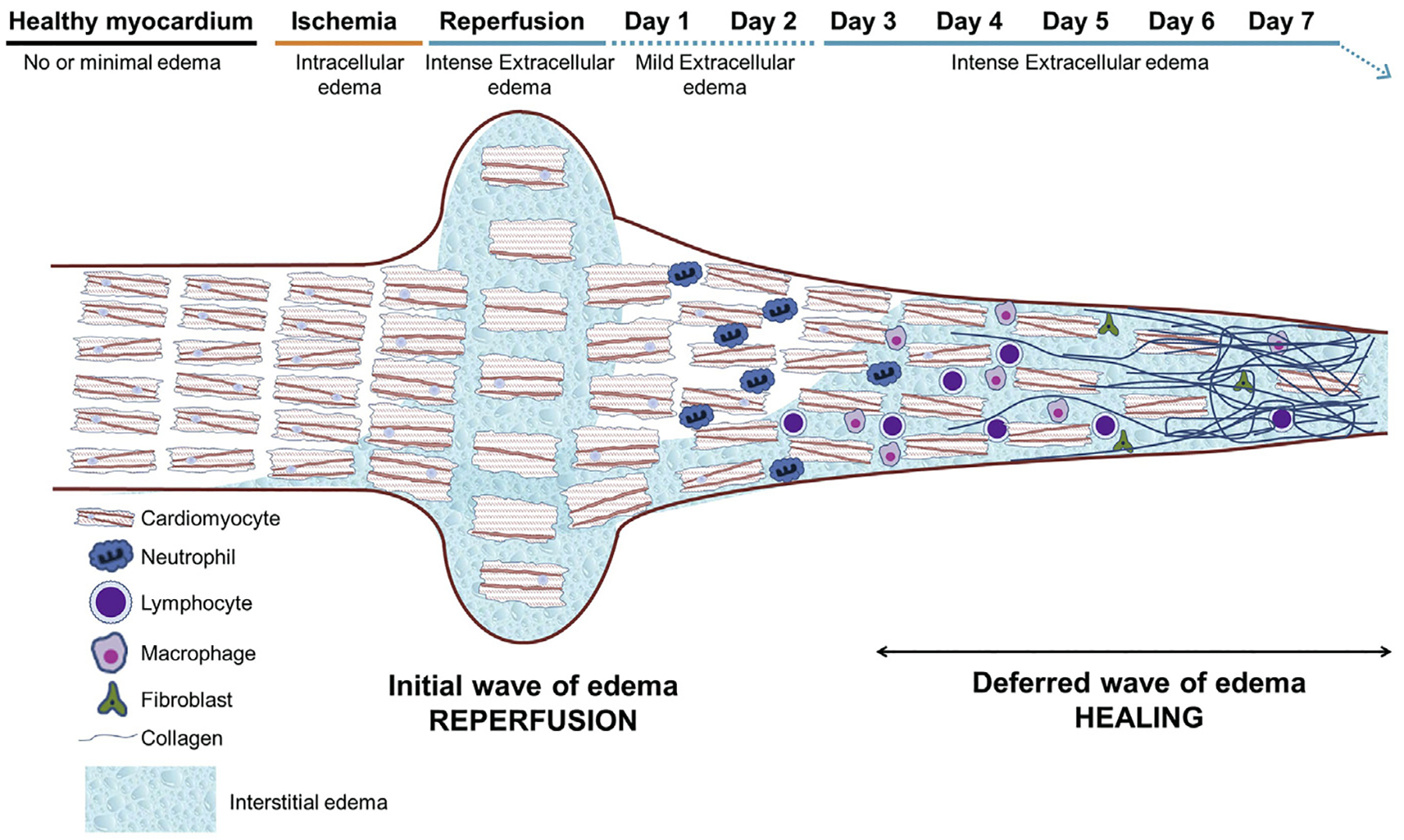
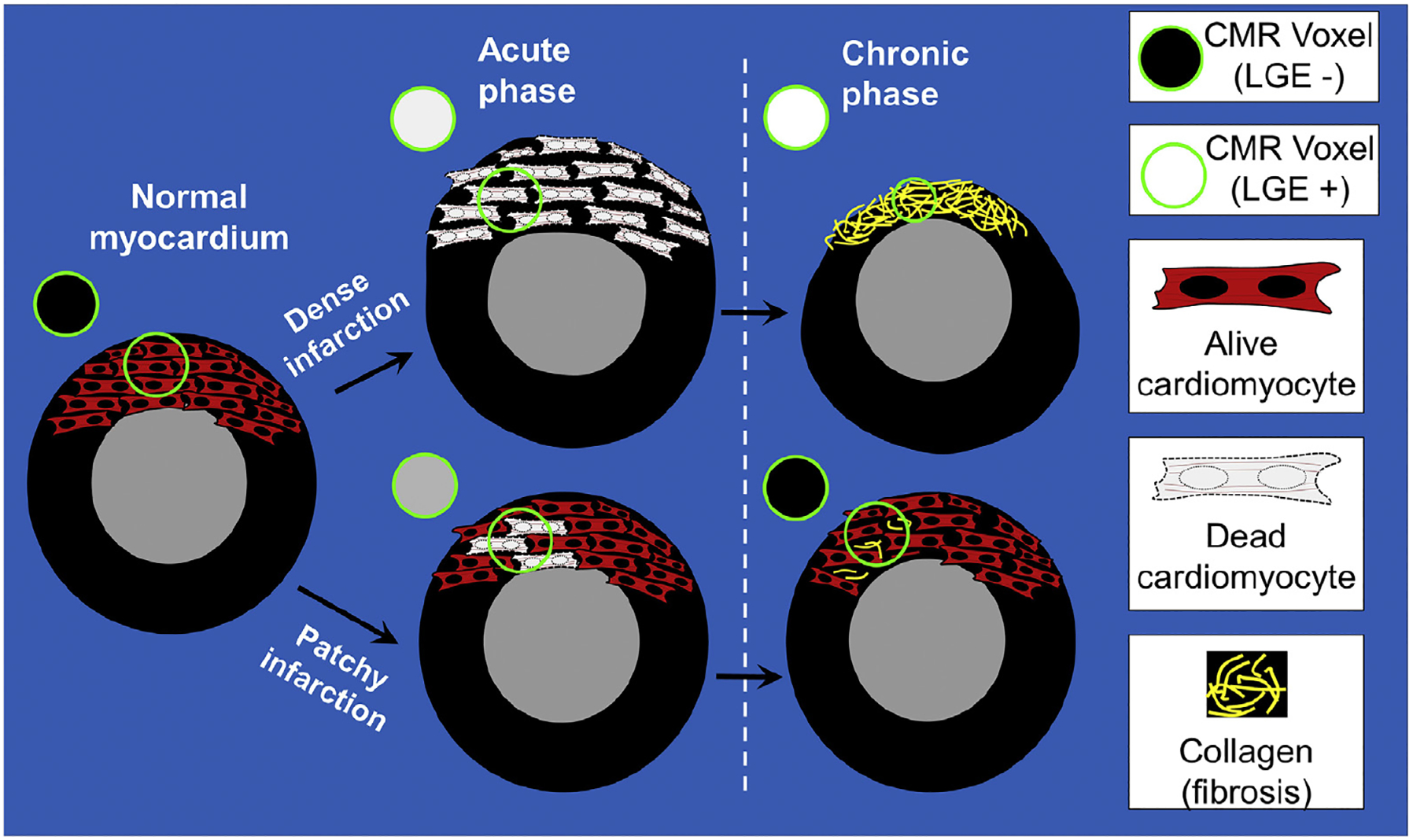
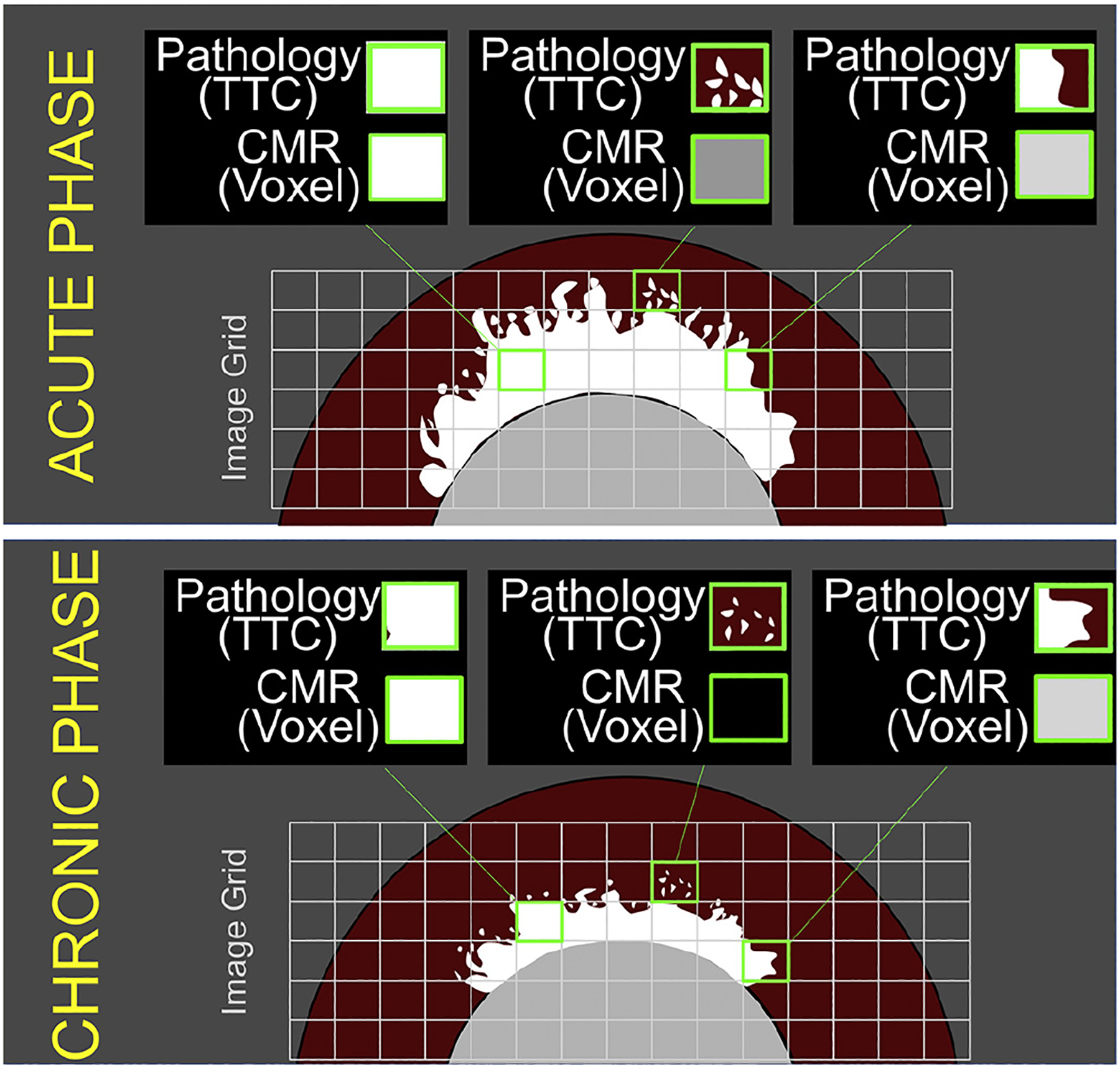
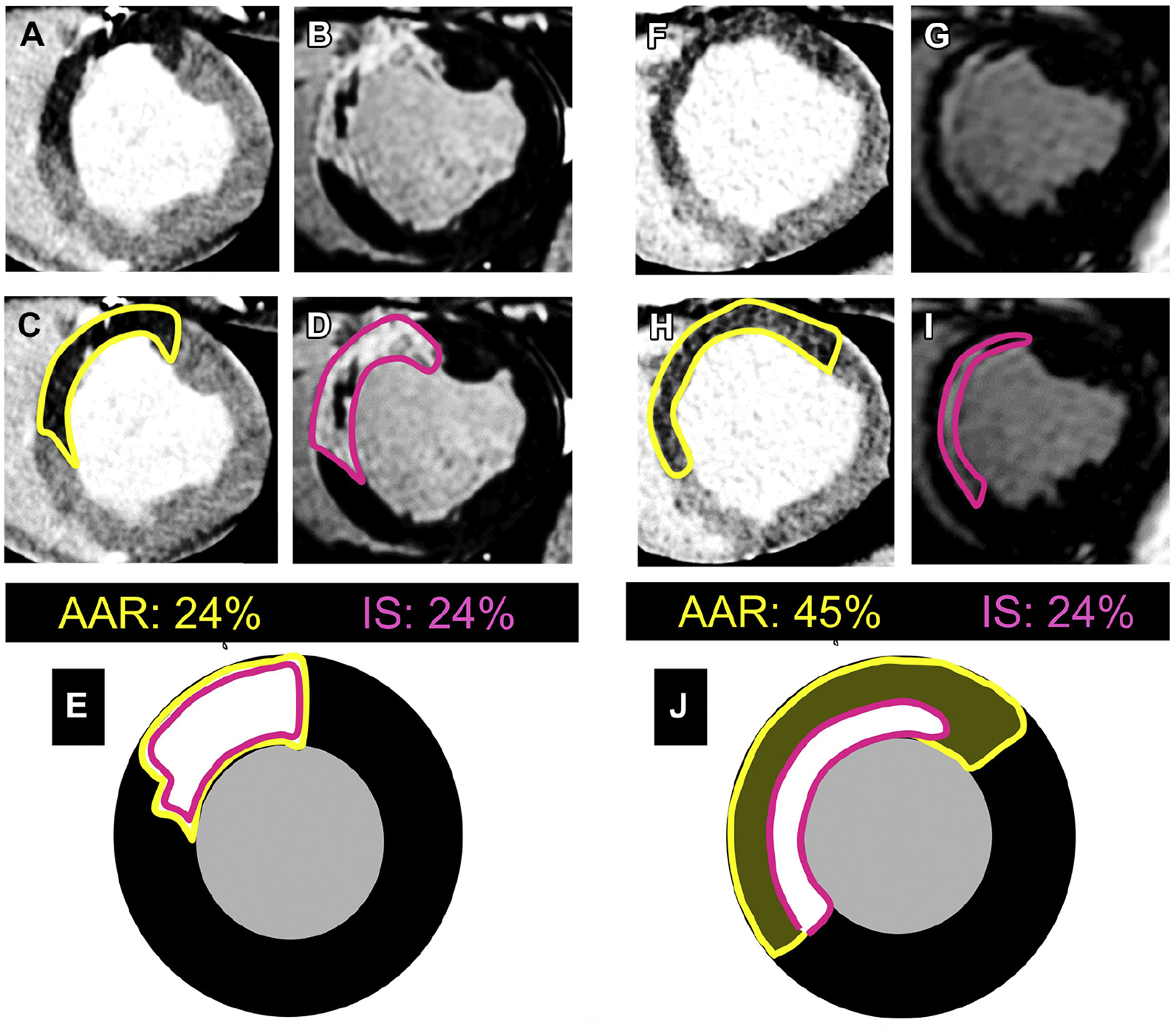
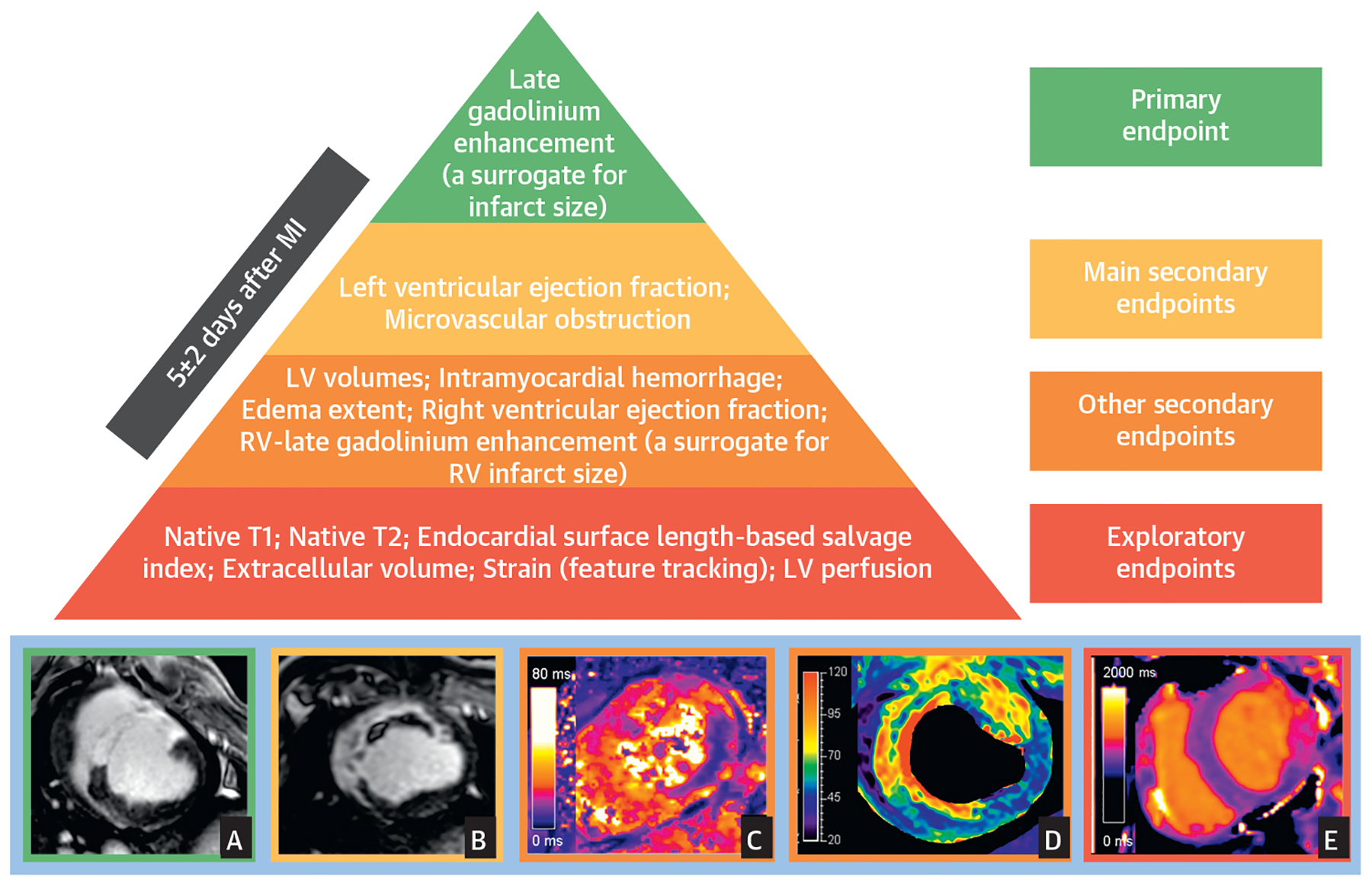
After a reperfused myocardial infarction (MI), dynamic tissue changes occur (edema, inflammation, microvascular obstruction, hemorrhage, cardiomyocyte necrosis, and ultimately replacement by fibrosis). The extension and magnitude of these changes contribute to long-term prognosis after MI. Cardiac magnetic resonance (CMR) is the gold-standard technique for noninvasive myocardial tissue characterization. CMR is also the preferred methodology for the identification of potential benefits associated with new cardioprotective strategies both in experimental and clinical trials. However, there is a wide heterogeneity in CMR methodologies used in experimental and clinical trials, including time of post-MI scan, acquisition protocols, and, more importantly, selection of endpoints. There is a need for standardization of these methodologies to improve the translation into a real clinical benefit. The main objective of this scientific expert panel consensus document is to provide recommendations for CMR endpoint selection in experimental and clinical trials based on pathophysiology and its association with hard outcomes.
Keywords: STEMI; area at risk; clinical trial; edema; endpoint; infarct size; magnetic resonance imaging; myocardial infarction.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ibanez B, Heusch G, Ovize M, Van de Werf F. Evolving therapies for myocardial ischemia/reperfusion injury. J Am Coll Cardiol 2015;65: 1454–71. - PubMed
-
- Messroghli DR, Moon JC, Ferreira VM, et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: a consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 2017;19:75. - PMC - PubMed
-
- Schulz-Menger J, Bluemke DA, Bremerich J, et al. Standardized image interpretation and post processing in cardiovascular magnetic resonance: Society for Cardiovascular Magnetic Resonance (SCMR) Board of Trustees Task Force on Standardized Post Processing. J Cardiovasc Magn Reson 2013;15:35. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
