

Current needs for the improved management of depressive disorder in community healthcare centres, Shenzhen, China: a view from primary care medical leaders
- PMID: 31297142
- PMCID: PMC6598358
- DOI: 10.1186/s13033-019-0300-0
Current needs for the improved management of depressive disorder in community healthcare centres, Shenzhen, China: a view from primary care medical leaders
Abstract
Background: The prevalence of depressive disorder in Shenzhen is higher than for any other city in China. Despite national health system reform to integrate mental health into primary care, the majority of depression cases continue to go unrecognized and untreated. Qualitative research was conducted with primary care medical leaders to describe the current clinical practice of depressive disorder in community healthcare centres (CHC) in Shenzhen and to explore the participants' perceptions of psychological, organizational and societal barriers and enablers to current practice with a view to identifying current needs for the improved care of depressive disorder in the community.
Methods: Seventeen semi-structured, audio-recorded interviews (approx. 1 h long) were conducted in Melbourne (n = 7) and Shenzhen (n = 10) with a convenience sample of primary care medical leaders who currently work in community healthcare centres (CHC) in Shenzhen and completed any one of the 3-month long, Melbourne-based, "Monash-Shenzhen Primary Healthcare Leaders Programs" conducted between 2015 and 2017. The interview guide was developed using the Theoretical Domain's Framework (TDF) and a directed content analysis (using Nvivo 11 software) was performed using English translations.
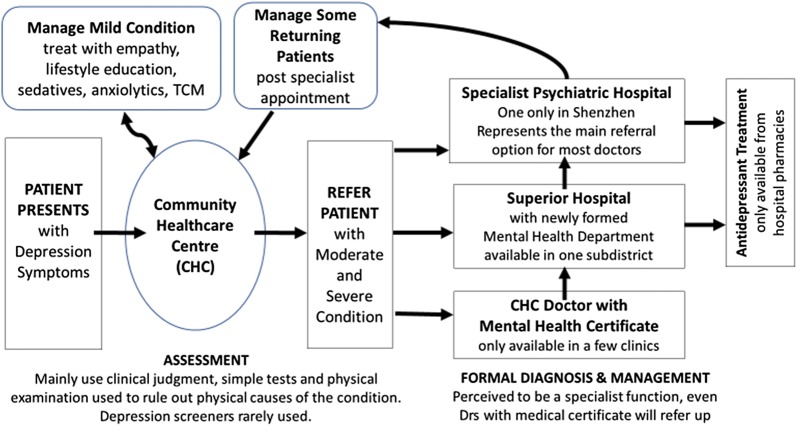
Results: Despite primary care medical leaders being aware of a mental health treatment gap and the benefits of early depression care for community wellbeing, depressive disorder was not perceived as a treatment priority in CHCs. Instead, hospital specialists were identified as holding primary responsibility for formal diagnosis and treatment initiation with primary care doctors providing early assessment and basic health education. Current needs for improved depression care included: (i) Improved professional development for primary care doctors with better access to diagnostic guidelines and tools, case-sharing and improved connection with mentors to overcome current low levels of treatment confidence. (ii) An improved consulting environment (e.g. allocated mental health resource; longer and private consultations; developed medical referral system; better access to antidepressants) which embraces mental health initiatives (e.g. development of mental health departments in local hospitals; future use of e-mental health; reimbursement for patients; doctors' incentives). (iii) Improved health literacy to overcome substantive mental health stigma in society and specific stigma directed towards the only public psychiatric hospital.
Conclusions: Whilst a multi-faceted approach is needed to improve depression care in community health centres in Shenzhen, this study highlights how appropriate mental health training is central to developing a robust work-force which can act as key agents in national healthcare reform. The cultural adaption of the depression component of the World Health Organisation's mental health gap intervention guide (mhGAP-IG.v2) could provide primary care doctors with a future training tool to develop their assessment skills and treatment confidence.
Keywords: Assessment; Barriers; China; Clinical practice; Common mental disorders; Community healthcare centres; Depression; Depressive disorder; Diagnosis; Enablers; Follow-up; Health system reform; Management; Mental Health GAP Intervention Guide (mhGAP-IG.v2); Mental health; Mental illness; Mental, neurological and substance use disorders (MNS); Primary care; Shenzhen; Theoretical Domain’s Framework (TDF).
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures

References
-
- Charlson FJ, Baxter AJ, Cheng HG, Shidhaye R, Whiteford HA. The burden of mental, neurological, and substance use disorders in China and India: a systematic analysis of community representative epidemiological studies. Lancet. 2016;388(10042):376–389. - PubMed
-
- Huang Y, Wang Y, Wang H, Liu Z, Yu X, Yan J, Yu Y, Kou C, Xu X, Lu J, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. - PubMed
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. DSM-5. 5. Philadelphia: American Psychiatric Association; 2013.
-
- Hu TW, He Y, Zhang M, Chen N. Economic costs of depression in China. Soc Psychiatry Psychiatr Epidemiol. 2007;42(2):110–116. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
