

How we treat glioblastoma
- PMID: 31297242
- PMCID: PMC6586206
- DOI: 10.1136/esmoopen-2019-000520
How we treat glioblastoma
Abstract
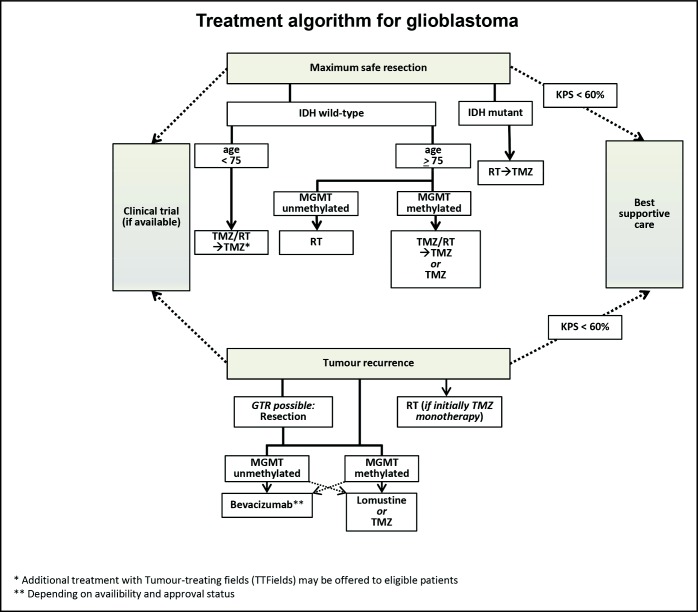
Glioblastoma is an intrinsic brain tumour thought to arise from neuroglial progenitor cells. Its incidence increases steadily with age. Males are moderately more often affected. Genetic predisposition and exposure to irradiation in childhood are the only established risk factors which, however, account only for a very small proportion of glioblastomas. Surgery as safely feasible not only to allow for tissue diagnosis but also to reduce tumour volume is usually the first therapeutic measure. Radiotherapy delivered to the tumour region with a safety margin has been demonstrated to roughly double survival four decades ago. Temozolomide given during radiotherapy followed by six cycles of maintenance chemotherapy was the first and so far only pharmacological treatment shown to prolong survival. Adding tumour-treating fields during maintenance, temozolomide chemotherapy has been reported to prolong survival. There is little evidence that any intervention at relapse improves outcome, but nitrosourea-based chemotherapy, commonly lomustine, is probably the most agreed on standard of care. Bevacizumab prolongs progression-free survival and probably quality of life in the first line or recurrent setting, but not overall survival, and is therefore not approved in the European Union. Immunotherapy remains experimental. Drugs in advanced clinical development include the programmed death 1 antibody, nivolumab, the antibody drug conjugate depatuxizumab directed to the epidermal growth factor receptor and the proteasome inhibitor marizomib.
Keywords: MGMT; chemotherapy; glioblastoma; radiotherapy; surgery.
Conflict of interest statement
Competing interests: MW has received research grants from Abbvie, Adastra, Dracen, Merck, Sharp & Dohme (MSD), Merck (EMD), Novocure, OGD2, Piqur and Roche and honoraria for lectures or advisory board participation or consulting from Abbvie, Basilea, Bristol Meyer Squibb, Celgene, Merck, Sharp & Dohme (MSD), Merck (EMD), Novocure, Orbus, Roche and Tocagen. ELR has received research grants from Mundipharma and Amgen and honoraria for lectures or advisory board participation from Abbvie, Daiichi Sankyo, Mundipharma and Novartis. MP has received honoraria for lectures, consultation or advisory board participation from the following for-profit companies: Bayer, Bristol-Myers Squibb, Novartis, Gerson Lehrman Group (GLG), CMC Contrast, GlaxoSmithKline, Mundipharma, Roche, Astra Zeneca, AbbVie, Lilly, Medahead, Daiichi Sankyo, Merck Sharp & Dome. JCT has received research grants from BrainLab and honoraria for lectures or consulting from BrainLAb and medac. PR has received honoraria for advisory board participation or lectures from Bristol-Myers Squibb, Covagen, Medac, MSD, Novartis, Novocure, Roche and Virometix.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
