

Heart failure from cancer therapy: can we prevent it?
- PMID: 31297946
- PMCID: PMC6676296
- DOI: 10.1002/ehf2.12493
Heart failure from cancer therapy: can we prevent it?
Abstract
Aims: Conventional cytotoxic chemotherapy is still among the most effective treatment options for many types of cancer. However, cardiotoxicity, notably the decrease in left ventricular function under these regimens, can impair prognosis. Thus, prevention and treatment of cardiotoxicity are crucial. The present meta-analysis aims to assess the efficacy of beta-blockers or angiotensin-converting enzyme (ACE) inhibitors/angiotensin II receptor blockers (ARBs) for prevention of cardiotoxicity.
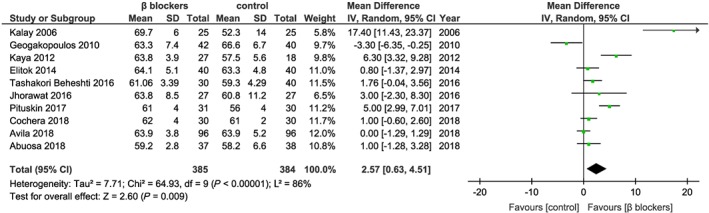
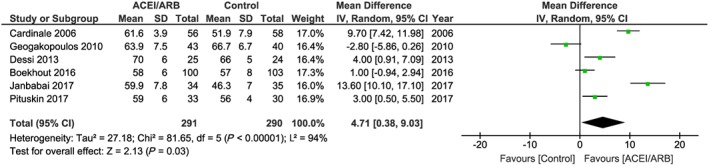
Methods and results: We systematically searched Pubmed, Cochrane, EMBASE, and Web of Science databases for randomized controlled trials published until February 2019. The analysis included randomized studies that reported on left ventricular ejection fraction (LVEF) after 6 months of chemotherapy in cancer patients who received beta-blockers or ACE inhibitors/ARBs for prevention of cardiotoxicity compared with controls. Studies on combination cardioprotective therapies were excluded from the analysis. The primary endpoint was prevention of a decrease in LVEF as defined by the individual study and as assessed by either transthoracic echocardiography or magnetic resonance imaging. We here show that patients under anthracycline-based chemotherapy have a moderate yet significant benefit in LVEF from beta-blockers or ACEs/ARBs. The beta-blocker analysis included 769 cancer patients, and the ACE inhibitors/ARBs analysis included a total of 581 cancer patients. The mean LVEF difference between the beta-blocker group and the control group was 2.57% (95% confidence interval 0.63-4.51, P = 0.009). The mean difference for ACE inhibitors/ARBs was 4.71% (95% confidence interval 0.38-9.03, P = 0.03). However, the beneficial effects throughout the studies were variable as documented by significant heterogeneity between the studies.
Conclusions: Systematic evidence is needed to solidly found recommendations for cardioprotective prevention during chemotherapy. Likewise, trials on other neurohumoral drugs (spironolactone) and lipid-lowering approaches are required to improve protection for cardio-oncology patients.
Keywords: Cardio-oncology; Cardiotoxicity; Meta-analysis.
© 2019 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Totzeck M, Schuler M, Stuschke M, Heusch G, Rassaf T. Cardio‐oncology—strategies for management of cancer‐therapy related cardiovascular disease. Int J Cardiol 2019; 280: 163–175. - PubMed
-
- Snipelisky D, Park JY, Lerman A, Mulvagh S, Lin G, Pereira N, Rodriguez‐Porcel M, Villarraga HR, Herrmann J. How to develop a cardio‐oncology clinic. Heart Fail Clin 2017; 13: 347–359. - PubMed
-
- Levis BE, Binkley PF, Shapiro CL. Cardiotoxic effects of anthracycline‐based therapy: what is the evidence and what are the potential harms? Lancet Oncol 2017; 18: e445–e456. - PubMed
-
- Mehta LS, Watson KE, Barac A, Beckie TM, Bittner V, Cruz‐Flores S, Dent S, Kondapalli L, Ky B, Okwuosa T, Pina IL, Volgman AS, American Heart Association Cardiovascular Disease in W, Special Populations Committee of the Council on Clinical C, Council on C, Stroke N, Council on Quality of C, Outcomes R . Cardiovascular disease and breast cancer: where these entities intersect: a scientific statement from the American Heart Association. Circulation 2018; 137: e30–e66. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
