

Spread and clinical severity of respiratory syncytial virus A genotype ON1 in Germany, 2011-2017
- PMID: 31299924
- PMCID: PMC6624929
- DOI: 10.1186/s12879-019-4266-y
Spread and clinical severity of respiratory syncytial virus A genotype ON1 in Germany, 2011-2017
Abstract
Background: The Respiratory Syncytial Virus (RSV) A genotype ON1, which was first detected in Ontario (Canada) in 2010/11, appeared in Germany in 2011/12. Preliminary observations suggested a higher clinical severity in children infected with this new genotype. We investigated spread and disease severity of RSV-A ON1 in pediatric in- and outpatient settings.
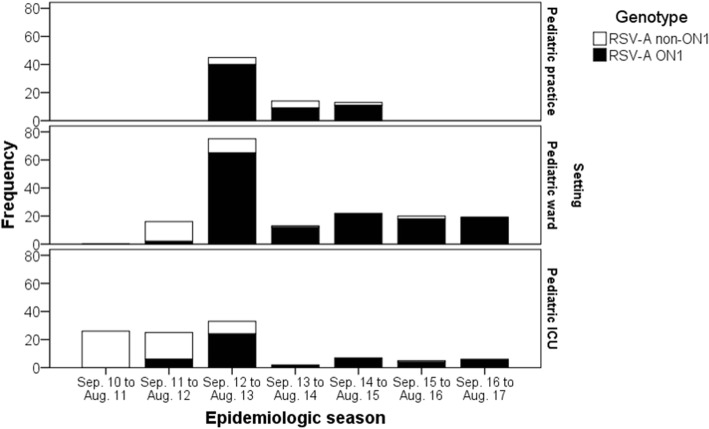
Methods: During 2010/11 to 2016/17, clinical characteristics and respiratory samples from children with acute respiratory tract infections (RTI) were obtained from ongoing surveillance studies in 33 pediatric practices (PP), one pediatric hospital ward (PW) and 23 pediatric intensive care units (PICU) in Germany. RSV was detected in the respiratory samples by PCR; genotypes were identified by sequencing. Within each setting, clinical severity markers were compared between RSV-A ON1 and RSV-A non-ON1 genotypes.
Results: A total of 603 children with RSV-RTI were included (132 children in PP, 288 in PW, and 183 in PICU). Of these children, 341 (56.6%) were infected with RSV-A, 235 (39.0%) with RSV-B, and one child (0.2%) with both RSV-A and RSV-B; in 26 (4.3%) children, the subtype could not be identified. In the 341 RSV-A positive samples, genotype ON1 was detected in 247 (72.4%), NA1 in 92 (26.9%), and GA5 in 2 children (0.6%). RSV-A ON1, rarely observed in 2011/12, was the predominant RSV-A genotype in all settings by 2012/13 and remained predominant until 2016/17. Children in PP or PW infected with RSV-A ON1 did not show a more severe clinical course of disease compared with RSV-A non-ON1 infections. In the PICU group, hospital stay was one day longer (median 8 days, inter-quartile range (IQR) 7-12 vs. 7 days, IQR 5-9; p = 0.02) and duration of oxygen treatment two days longer (median 6 days, IQR 4-9 vs. 4 days, IQR 2-6; p = 0.03) for children infected with RSV-A ON1.
Conclusions: In children, RSV-A ON1 largely replaced RSV-A non-ON1 genotypes within two seasons and remained the predominant RSV-A genotype in Germany during subsequent seasons. A higher clinical severity of RSV-A ON1 was observed within the group of children receiving PICU treatment, whereas in other settings clinical severity of RSV-A ON1 and non-ON1 genotypes was largely similar.
Keywords: Children; Disease severity; Epidemiology; RSV-A ON1; Respiratory tract infection.
Conflict of interest statement
AS received research grants, speaker’s fees, and/or fees for participation in advisory board meetings and travelling grants from GlaxoSmithKline GmbH Co.KG (Germany) and Pfizer Pharma GmbH (Germany). JGL received research grants, speaker’s fees, and fees for participation in advisory board meetings from GlaxoSmithKline GmbH Co.KG (Germany), Pfizer Pharma GmbH (Germany), SPMSD and MSD. The other authors declare that they have no competing interests.
Figures
References
-
- Shi T, McAllister DA, O'Brien KL, Simoes EAF, Madhi SA, Gessner BD, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390:946–958. doi: 10.1016/S0140-6736(17)30938-8. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
