

Postoperative complications and nutritional status between uncut Roux-en-Y anastomosis and Billroth II anastomosis after D2 distal gastrectomy: a study protocol for a multicenter randomized controlled trial
- PMID: 31300019
- PMCID: PMC6626339
- DOI: 10.1186/s13063-019-3531-0
Postoperative complications and nutritional status between uncut Roux-en-Y anastomosis and Billroth II anastomosis after D2 distal gastrectomy: a study protocol for a multicenter randomized controlled trial
Abstract
Background: Gastric cancer is the fourth most common malignant disease worldwide, with lower one-third gastric cancer the most common type. Distal gastrectomy with D2 lymph node dissection was recommended as a standard surgery for distal gastric cancer patients. However, some controversy remains about the anastomosis of the residual stomach and the intestine. The objectives of this trial are to test the hypothesis that uncut Roux-en-Y anastomosis can reduce postoperative complications and improve nutritional status more effectively than Billroth II anastomosis in gastric cancer patients after D2 gastrectomy.
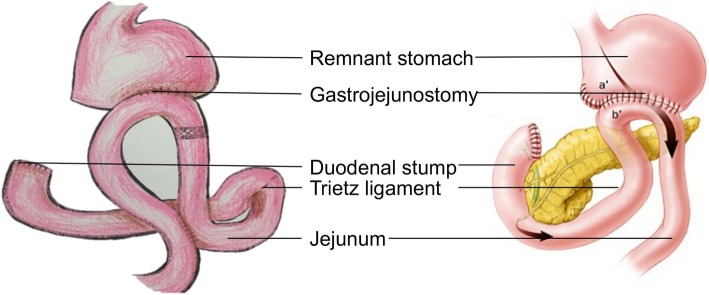
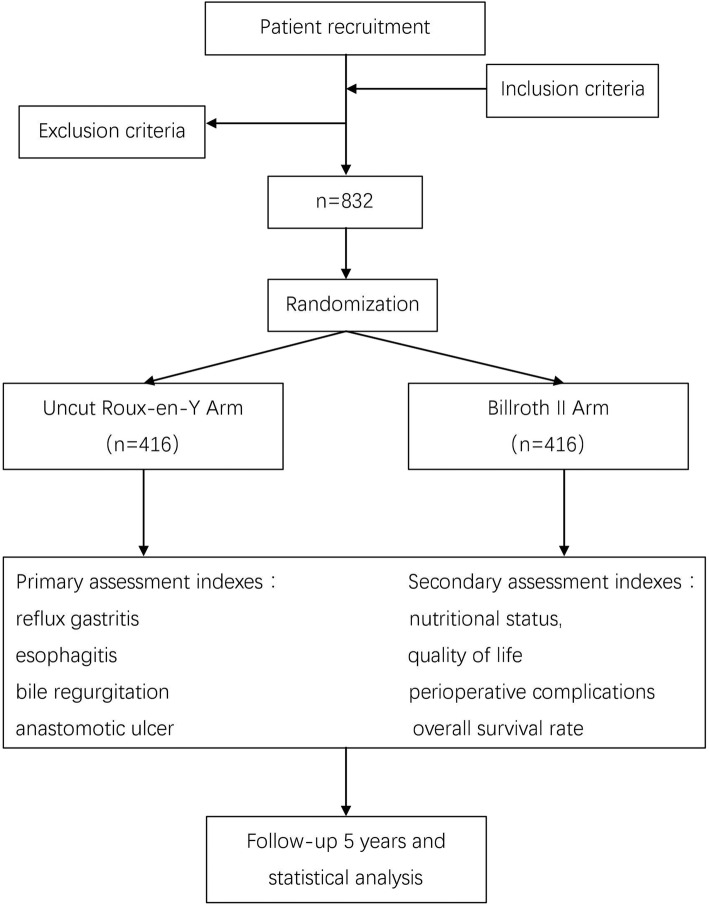
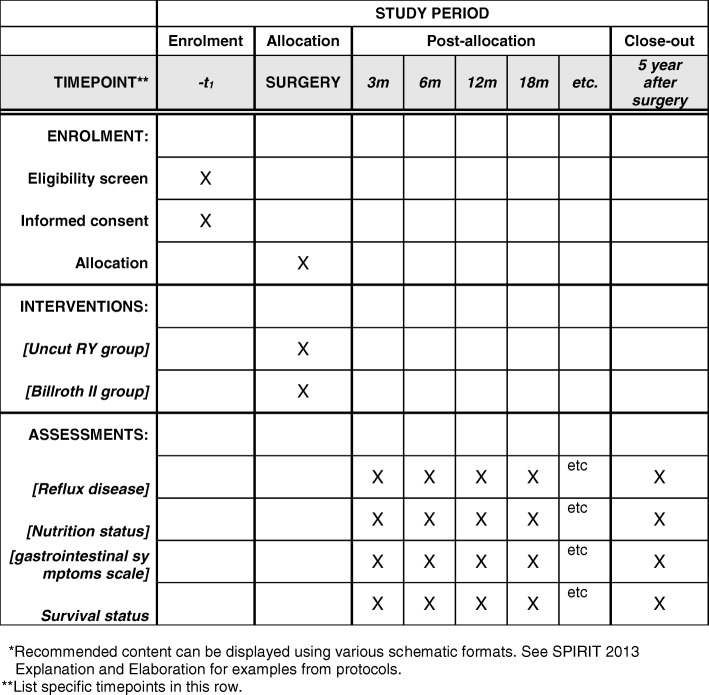
Methods/design: This multi-center, prospective, phase III, randomized controlled trial will compare the efficacy of uncut Roux-en-Y anastomosis versus Billroth II anastomosis in phase I-III patients with initial treatment of radical distal gastrectomy. Patients will be randomized to undergo either the intervention (uncut Roux-en-Y anastomosis) or the control (Billroth II anastomosis). We will recruit 832 patients who meet the trial eligibility criteria and will follow the patients after surgery to observe postoperative complications and nutrition status for 5 years. The primary assessment indices of the study are reflux gastritis, esophagitis, bile regurgitation, and anastomotic ulcer. The secondary assessment indices are nutritional status, quality of life, perioperative complications, overall survival rate, and others. When the number of cases reaches 400, an interim analysis will be performed to identify any evidence of definite superiority of the experimental intervention.
Discussion: We aim to test the hypothesis that uncut Roux-en-Y anastomosis can reduce postoperative complications and improve nutritional status more than Billroth II anastomosis in gastric cancer patients after D2 gastrectomy. The results of the trial will contribute to the best evidence on which to base the reconstruction of distal gastrectomy.
Trial registration: Chinese Southern Gastric Cancer Conference CSGC002 Trial. ClinicalTrials.gov, NCT02763878 . Registered on 5 May 2016.
Keywords: Billroth II anastomosis; D2 distal gastrectomy; Nutritional status; Uncut Roux-en-Y anastomosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
