

Symptomatic malignant spinal cord compression in children: a single-center experience
- PMID: 31300063
- PMCID: PMC6626347
- DOI: 10.1186/s13052-019-0671-5
Symptomatic malignant spinal cord compression in children: a single-center experience
Abstract
Background: Malignant spinal cord compression (MSCC) is associated withpoor prognosis and may lead to permanent paralysis, sensory loss, and sphincter dysfunction. Very limited data are available on incidence and etiology of MSCC in pediatric population. We aimed to examine etiology, clinical presentation and treatment of pediatric patient with MSCC admitted to the Santobono-Pausilipon Children's Hospital, Naples, Italy.
Methods: Forty-four children under 18 yearsadmitedsince 2007 and assessed for MSCC clinical presentations, evaluation, and treatment.were retrospectively collected from our institutional pediatric oncology and neurosurgery database.
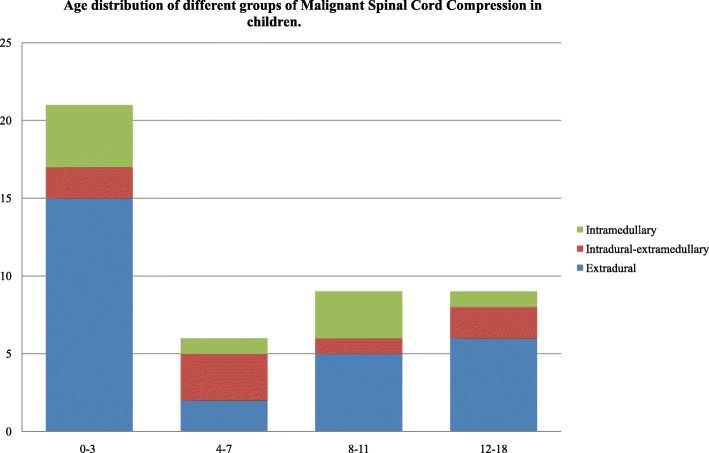
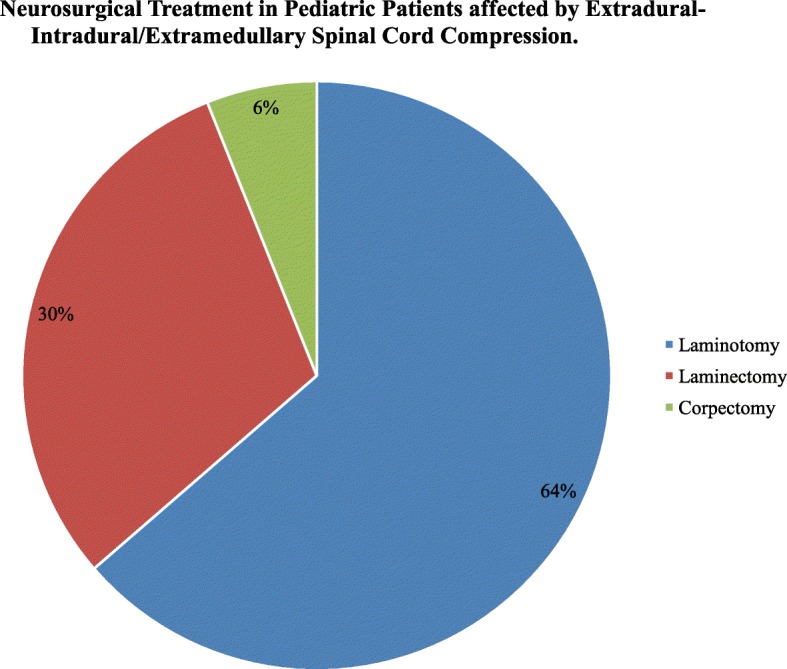
Results: The median age at time of MSCC diagnosis was 52 months, with a peak in young (≤3 years) patients. The leading cause of MSCC was extramedullary tumors (63.6%), in particular neuroblastoma (27.2%) followed by Ewing sarcomas (15.9%). Cord compression was the presenting feature of a new malignancy in 33 (75%) patients, and a consequence of metastatic disease progression or relapse in the remaining 11 (25%) patients. Motor deficit was the initial symptoms of spinal compression in all patients, while pain was present in about 60% of patients, followed by sphincteric deficit (43.2%). The primary tumor site was located in the neck in 3 (6.8%) patients, thorax in 16 (36.4%), cervico-thoracic region in 3 (6.8%), thoraco-lumbar region in 8 (18.2%), abdomen in 5 (11.4%), lumbar-sacral region in 7 (15.9%) and thoracic-lumbar-sacral region in 1 (2.3%). The median length of the interval between symptom onset and tumor diagnosis varied widely from 0 to 360 days in the entire population, however this interval was significantly shorter in patients with known neoplasia in comparisonto patients with new diagnosis (at relapse 7 days [interquartile range 3-10] vs at diagnosis 23 days [7-60]). Pre and post-operative spine magnetic resonance imagingwas performed in all cases, and most(95%) patients underwent neurosurgical treatment as first treatment. Severe motor deficit was associated with younger age and severe motor deficit at diagnosis was associated withworst motor outcomes at discharge from neurosurgery. Patients with progression or relapsed disease showed a worst prognosis, while the majority of patients (70.5%) were alive at 5 years after diagnosis.
Conclusions: The natural history of MSCC in children is associated to permanent paralysis, sensory loss, and sphincter dysfunction, thus prompt diagnosis and correct management are needed to minimize morbidity. Treatment strategies differed widely among cancer types and study groups in the absence of optimal evidence-based treatment guidelines. When the diagnosis is uncertain, surgery provides an opportunity to biopsy the lesion in addition to treating the mass.
Keywords: Extramedullary; Intradural; Intramedullary; Motor deficit; Pain; Sphincter dysfunction; Spinal cord compression.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
