

Incidence, Risk Factors, and Outcomes of Ventilator-Associated Pneumonia in Traumatic Brain Injury: A Meta-analysis
- PMID: 31300956
- PMCID: PMC7223912
- DOI: 10.1007/s12028-019-00773-w
Incidence, Risk Factors, and Outcomes of Ventilator-Associated Pneumonia in Traumatic Brain Injury: A Meta-analysis
Abstract
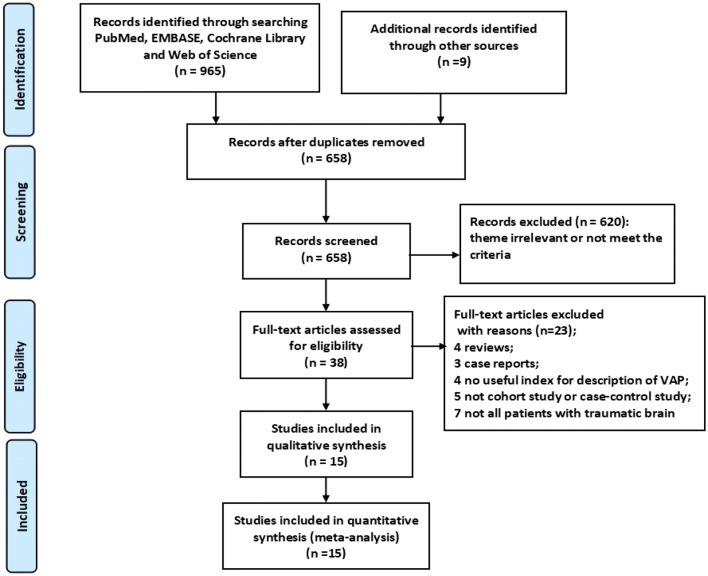
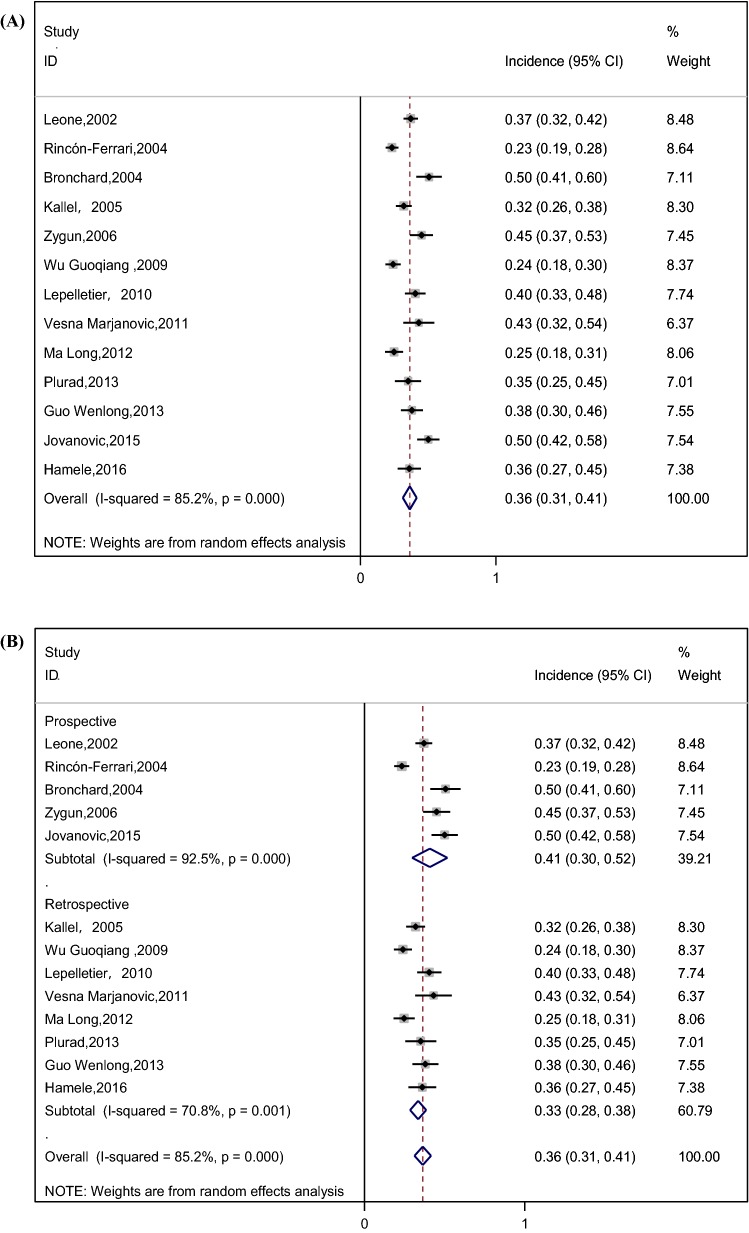
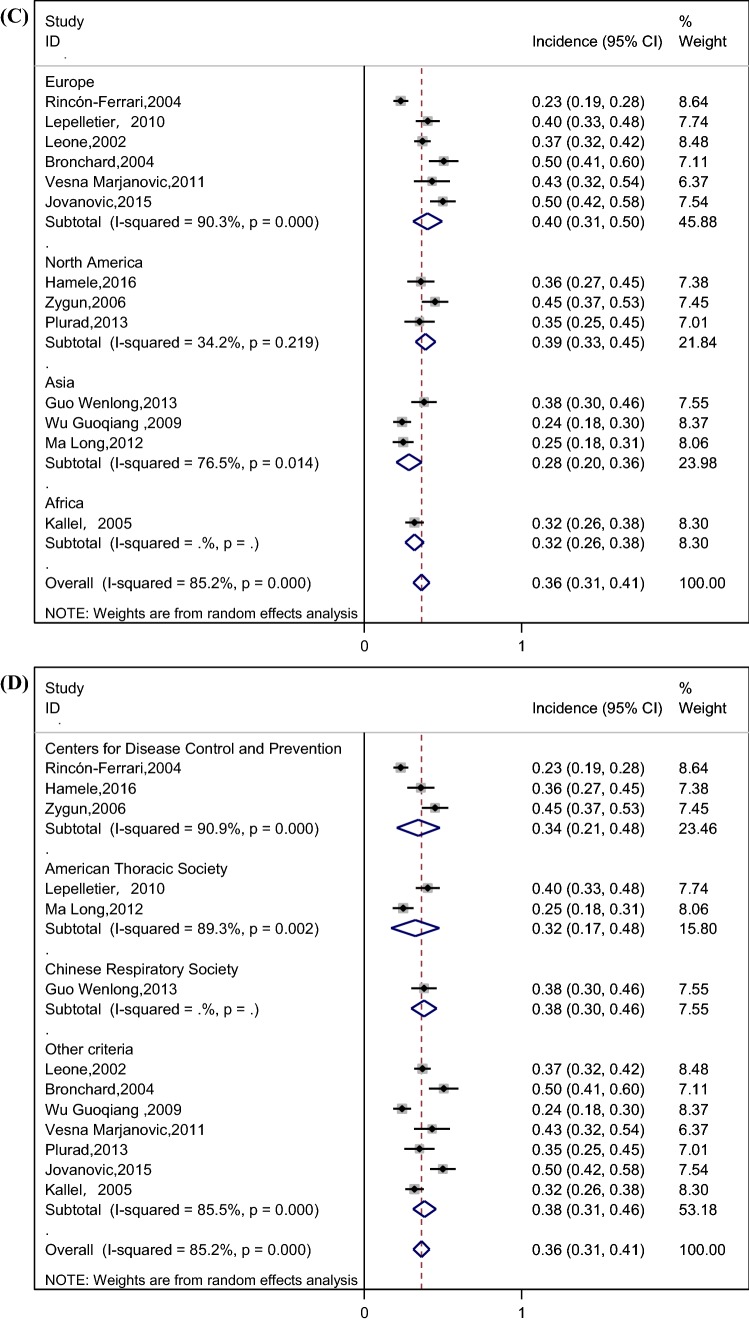
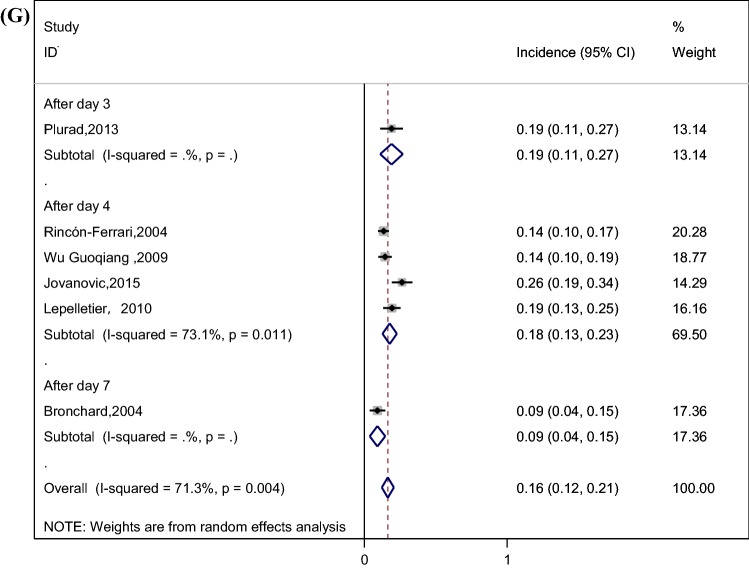
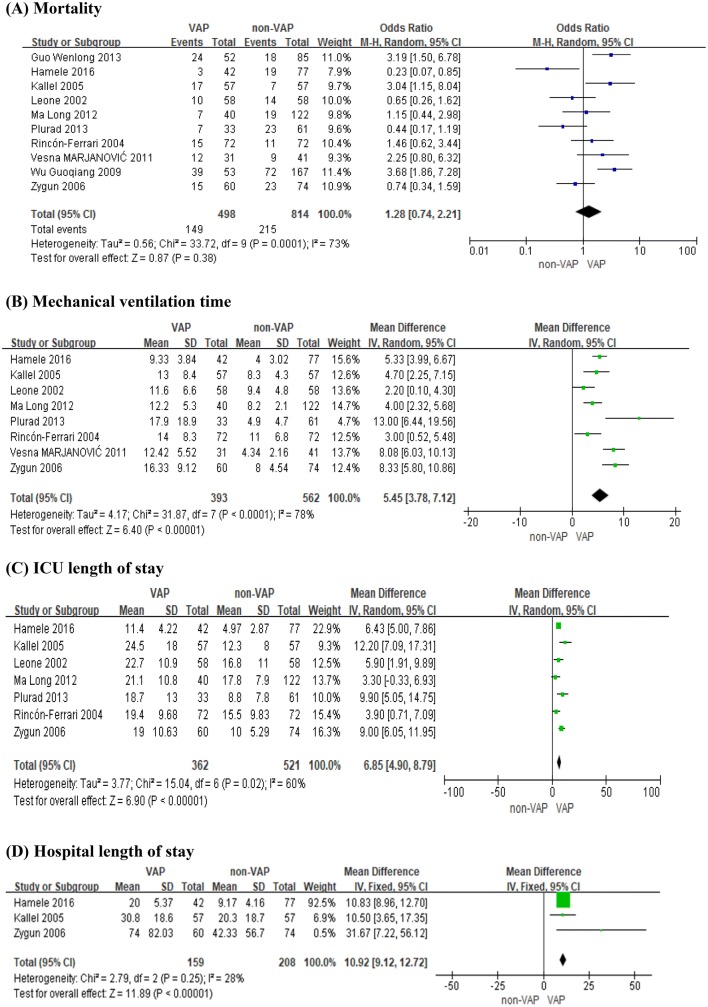
Ventilator-associated pneumonia (VAP) is one of the most severe complications in patients with traumatic brain injury (TBI) and is considered a risk factor for poor outcomes. However, the incidence of VAP among patients with TBI reported in studies varies widely. What is more, the risk factors and outcomes of VAP are controversial. This study estimates the incidence, risk factors, and outcomes of VAP in patients with TBI and provides evidence for prevention and treatment. PubMed, EMBASE, Cochrane Library, and Web of Science databases were searched from the earliest records to May 2018. Data involving the incidence, risk factors, and outcomes were extracted for meta-analysis. The results showed that the incidence of VAP was 36% (95% confidence interval (CI) 31-41%); risk factors analyses showed that smoking [odds ratio (OR) 2.13; 95% CI 1.16-3.92], tracheostomy (OR 9.55; 95% CI 3.24-28.17), blood transfusion on admission (OR 2.54; 95% CI 1.24-5.18), barbiturate infusion (OR 3.52; 95% CI 1.68-7.40), injury severity score (OR 4.65; 95% CI 1.96-7.34), and head abbreviated injury scale (OR 2.99; 95% CI 1.66-5.37) were related to the occurrence of VAP. When patients developed VAP, mechanical ventilation time (OR 5.45; 95% CI 3.78-7.12), ICU length of stay (OR 6.85; 95% CI 4.90-8.79), and hospital length of stay (OR 10.92; 95% CI 9.12-12.72) were significantly increased. However, VAP was not associated with an increased risk of mortality (OR 1.28; 95% CI 0.74-2.21). VAP is common in patients with TBI. It is affected by a series of factors and has a poor prognosis.
Keywords: Incidence; Outcome; Risk factors; Traumatic brain injury; Ventilator-associated pneumonia.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
-
- Ngubane T. Mechanical ventilation and the injured brain. South Afr J Anaesth Analg. 2011;17(1):76–80.
-
- Pileggi C, Bianco A, Flotta D, Nobile CGA, Pavia M. Prevention of ventilator-associated pneumonia, mortality and all intensive care unit acquired infections by topically applied antimicrobial or antiseptic agents: a meta-analysis of randomized controlled trials in intensive care units. Crit Care. 2011;15(3):R155. doi: 10.1186/cc10285. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
