

Transfers to Hemodialysis Among US Patients Initiating Renal Replacement Therapy With Peritoneal Dialysis
- PMID: 31301926
- PMCID: PMC6815249
- DOI: 10.1053/j.ajkd.2019.05.014
Transfers to Hemodialysis Among US Patients Initiating Renal Replacement Therapy With Peritoneal Dialysis
Abstract
Rationale & objective: Identifying patients who are likely to transfer from peritoneal dialysis (PD) to hemodialysis (HD) before transition could improve their subsequent care. This study developed a prediction tool for transition from PD to HD.
Study design: Retrospective cohort study.
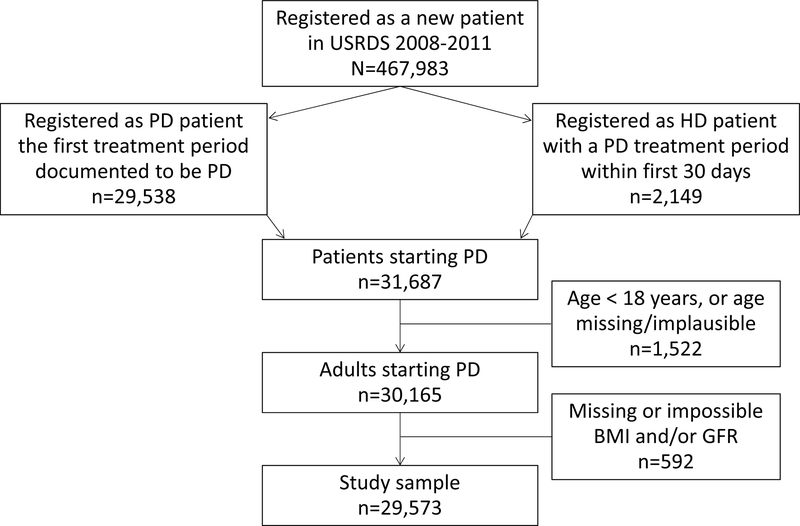
Setting & participants: Adults initiating PD between January 2008 and December 2011, followed up through June 2015, for whom data were available in the US Renal Data System (USRDS).
Predictors: Clinical characteristics at PD initiation and peritonitis claims.
Outcomes: Transfer to HD, with the competing outcomes of death and kidney transplantation.
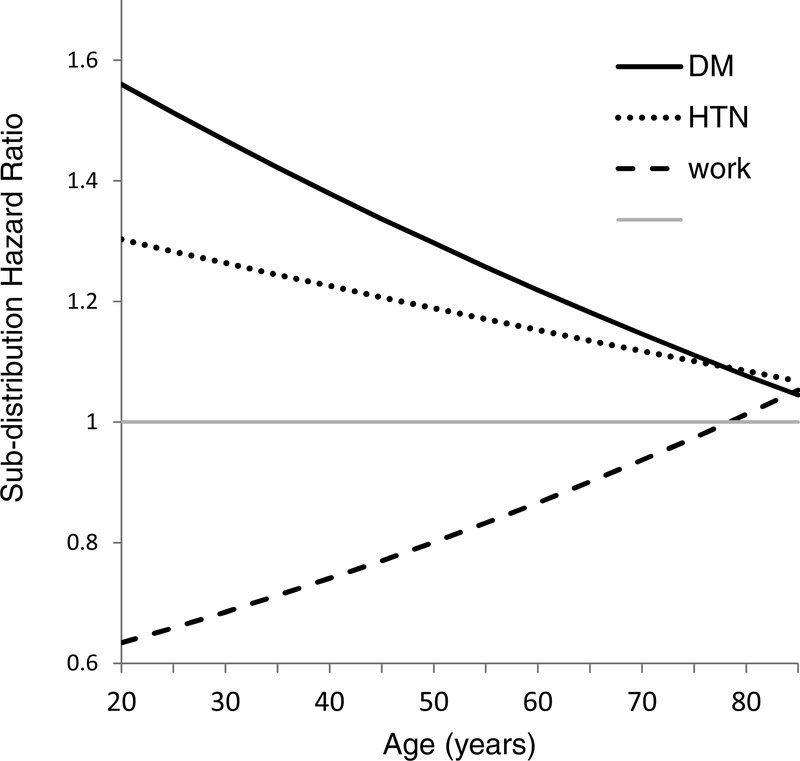
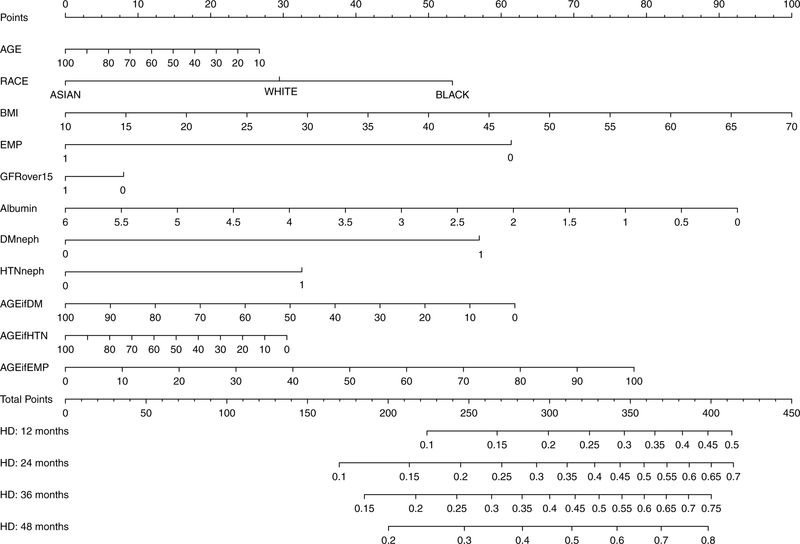
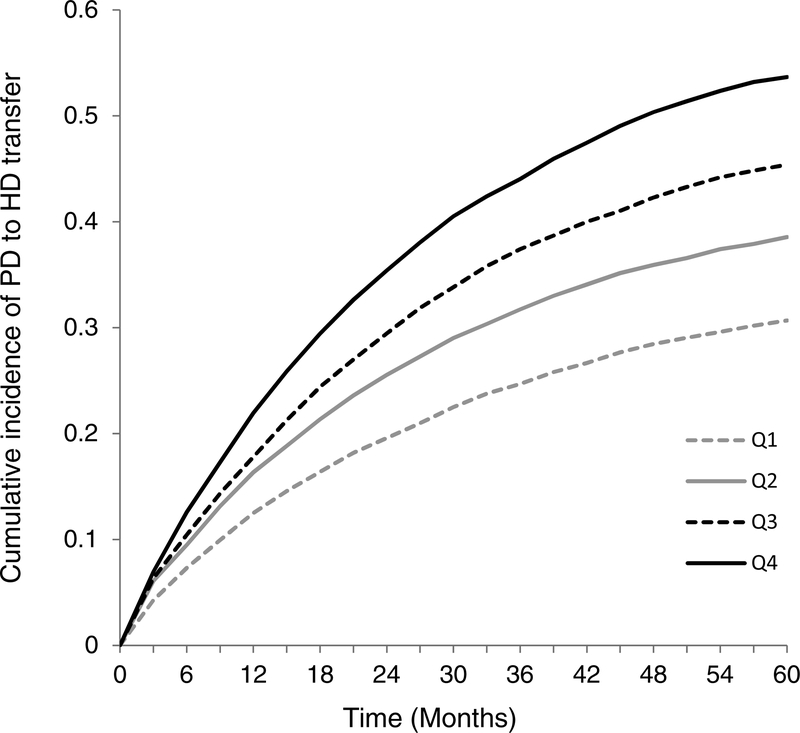
Analytical approach: Outcomes were ascertained from USRDS treatment history files. Subdistribution hazards (competing-risk) models were fit using clinical characteristics at PD initiation. A nomogram was developed to classify patient risk at 1, 2, 3, and 4 years. These data were used to generate quartiles of HD transfer risk; this quartile score was incorporated into a cause-specific hazards model that additionally included a time-dependent variable for peritonitis.
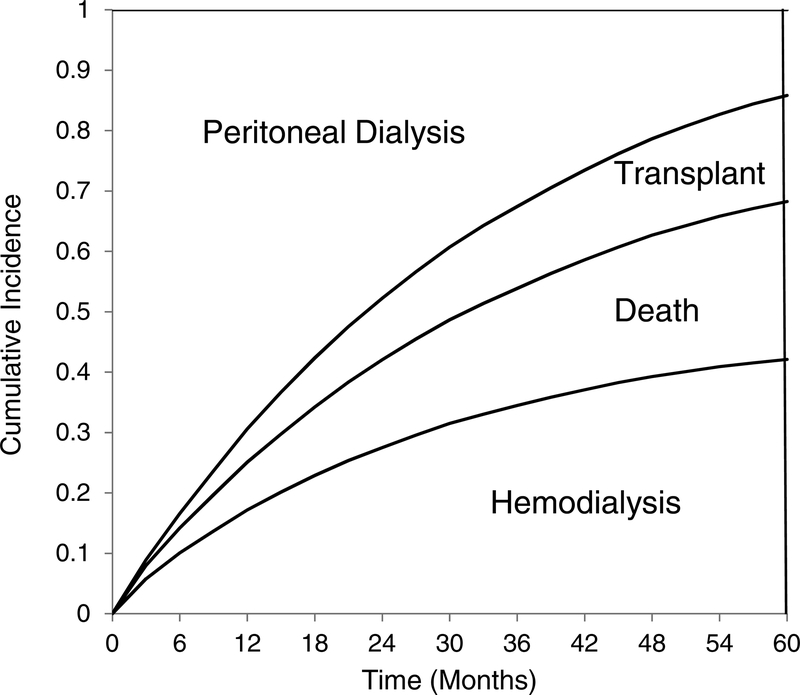
Results: 29,573 incident PD patients were followed up for a median of 21.6 (interquartile range, 9.0-42.3) months, during which 41.2% transferred to HD, 25.9% died, 17.1% underwent kidney transplantation, and the rest were followed up to the study end in June 2015. Claims for peritonitis were present in 11,733 (40.2%) patients. The proportion of patients still receiving PD decreased to <50% at 22.6 months and 14.2% at 5 years. Peritonitis was associated with a higher rate of HD transfer (HR, 1.82; 95% CI, 1.76-1.89; P < 0.001), as were higher quartile scores of HD transfer risk (HRs of 1.31 [95% CI, 1.25-1.37), 1.51 [95% CI, 1.45-1.58], and 1.78 [95% CI, 1.71-1.86] for quartiles 2, 3, and 4 compared to quartile 1 [P < 0.001 for all]).
Limitations: Observational data, reliant on the Medical Evidence Report and Medicare claims.
Conclusions: A large majority of the patients who initiated renal replacement therapy with PD discontinued this modality within 5 years. Transfer to HD was the most common outcome. Patient characteristics and comorbid diseases influenced the probability of HD transfer, death, and transplantation, as did episodes of peritonitis.
Keywords: HD transfer; Peritoneal dialysis (PD); competing risks; dialysis modality; hemodialysis (HD); modality switch; nomogram; prediction; prediction tool; prognosis; renal replacement therapy (RRT).
Copyright © 2019 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Characteristics Associated With Peritoneal Dialysis Technique Failure: Are We Asking the Right Questions?Am J Kidney Dis. 2019 Nov;74(5):586-588. doi: 10.1053/j.ajkd.2019.07.002. Epub 2019 Sep 9. Am J Kidney Dis. 2019. PMID: 31515139 No abstract available.
References
-
- Devoe DJ, Wong B, James MT, Ravani P, Oliver MJ, Barnieh L, et al. Patient education and peritoneal dialysis modality selection: A systematic review and meta-analysis. Am J Kidney Dis 68(3): 422–33, 2016 - PubMed
-
- Robinski M, Mau W, Wienke A, Girndt M. The choice of renal replacement therapy (CORETH) project: dialysis patients’ psychosocial characteristic and treatment satisfaction. Nephrol Dial Transplant 32(2): 315–24, 2017 - PubMed
-
- Dahlerus C, Quinn M, Messersmith E, Lachance L, Subramanian L, Perry E, et al. Patient perspectives on the choice of dialysis modality: Results from the Empowering Patients on Choices for Renal Replacement Therapy (EPOCH-RRT) Study. Am J Kidney Dis 68(6): 901–10, 2016 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
