

Effect of Bariatric Surgery on Male Sexual Function: A Meta-Analysis and Systematic Review
- PMID: 31302076
- PMCID: PMC6728768
- DOI: 10.1016/j.esxm.2019.06.003
Effect of Bariatric Surgery on Male Sexual Function: A Meta-Analysis and Systematic Review
Abstract
Introduction: Obesity is a worldwide public health issue with serious psychological and social impacts. Erectile dysfunction is also a common clinical condition, and obesity is one of its main risk factors.
Objective: The objective of this study was to systematically evaluate the effect of bariatric surgery on male sexual function.
Methods: A systematical research was carried out in Medline via PubMed, EMBASE, Cochrane Library, and Web of Science up to March 16, 2019, to identify published articles related to bariatric surgery and male sexual function in men. Two reviewers screened literature, extracted data, and assessed the quality of included studies. I2 index was applied to estimate the heterogeneity. All analyses were done using RevMan5.3 and Stata14.
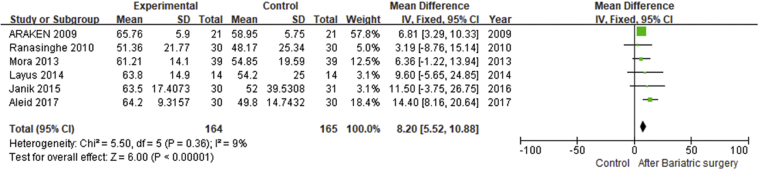
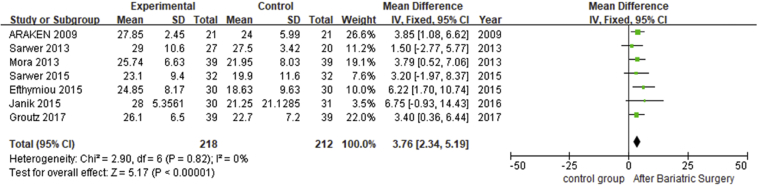
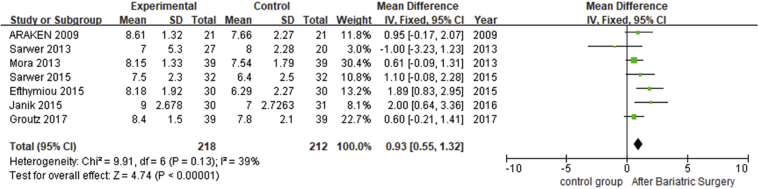
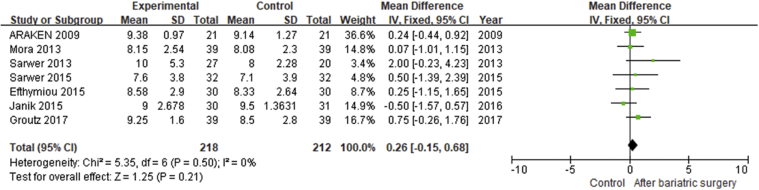
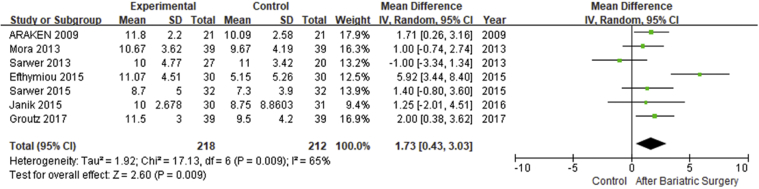
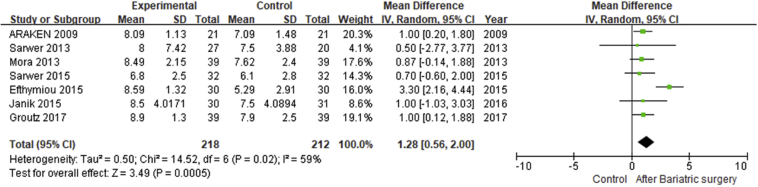
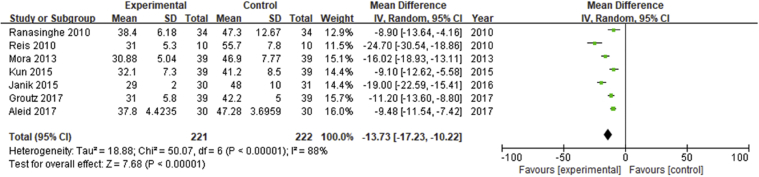
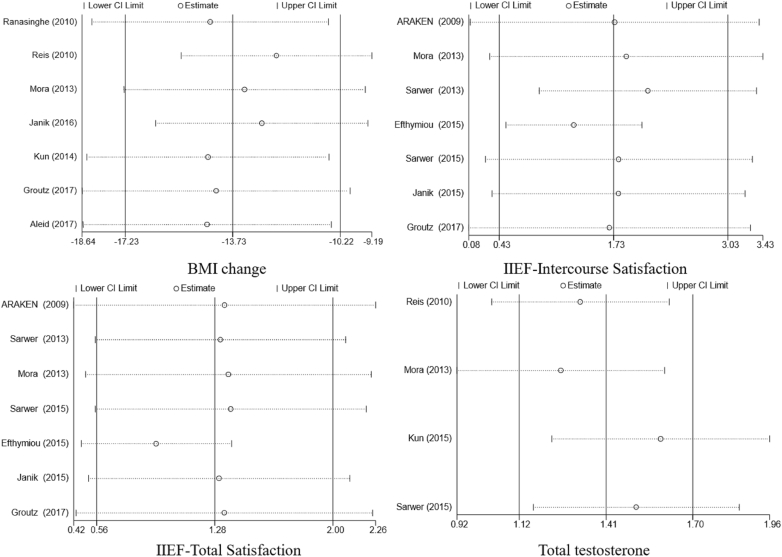
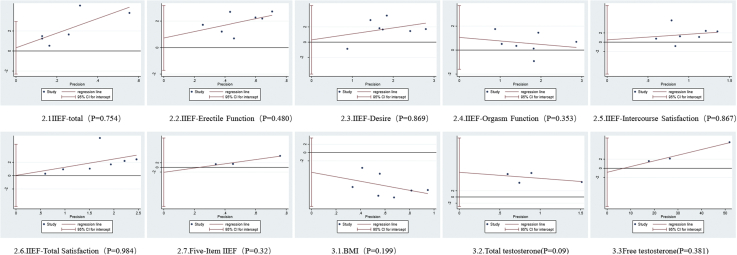
Results: A total of 12 studies involving 420 participants were included. Analysis showed that bariatric surgery significantly reduced body mass index in morbidly obese patients (mean difference [MD] = -13.73; 95% CI -17.23 to -10.22; P < .00001). From 10 studies that reported the International Index of Erectile Function (IIEF) score, bariatric surgery led to a significant increase in IIEF-total score (MD = 8.2; 95% CI = 5.52-10.88; P < .00001), and erectile function score (MD = 3.76; 95% CI = 2.34-5.19; P < .00001), sexual desire (MD = 0.93; 95% CI = 0.55-1.32; P < .00001), sexual intercourse satisfaction (MD = 1.73; 95% CI = 0.43-3.03; P < .01), and total satisfaction (MD = 1.28; 95% CI = 0.56-2.00; P = .0005) were also significantly improved. However, bariatric surgery did not affect orgasm function (MD = 0.26; 95% CI = -0.15 to 0.68; P = .21). Three studies that reported the IIEF-5 score also showed a significant improvement of erectile function (MD = 5.45; 95% CI = 3.38-7.52; P < .00001).
Conclusions: Bariatric surgery could improve the erectile function, sexual desire, sexual intercourse satisfaction, and total satisfaction in morbidly obese men. Due to limited data on body mass index and hormone levels, our meta-analysis had some limitations. More clinical studies are needed to further explore the relationship between bariatric surgery and male sexual function. Xu J, Wu Q, Zhang Y, et al. Effect of Bariatric Surgery on Male Sexual Function: A Meta-Analysis and Systematic Review. Sex Med 2019;7:270-281.
Keywords: Bariatric Surgery; Erectile Function; Meta-Analysis; Obesity; Sexual Function; Systematic Review.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures



Similar articles
-
Influence of Bariatric Surgery on Erectile Dysfunction-a Systematic Review and Meta-Analysis.Obes Surg. 2023 Jun;33(6):1652-1658. doi: 10.1007/s11695-023-06572-9. Epub 2023 Apr 22. Obes Surg. 2023. PMID: 37086370 Free PMC article.
-
The relationships between bariatric surgery and sexual function: current evidence based medicine.BMC Urol. 2020 Oct 2;20(1):150. doi: 10.1186/s12894-020-00707-1. BMC Urol. 2020. PMID: 33008406 Free PMC article.
-
Impact of Bariatric Surgery on Male Sex Hormones and Sperm Quality: a Systematic Review and Meta-Analysis.Obes Surg. 2019 Jan;29(1):334-346. doi: 10.1007/s11695-018-3557-5. Obes Surg. 2019. PMID: 30382463
-
Meta-analysis of Results of Testosterone Therapy on Sexual Function Based on International Index of Erectile Function Scores.Eur Urol. 2017 Dec;72(6):1000-1011. doi: 10.1016/j.eururo.2017.03.032. Epub 2017 Apr 20. Eur Urol. 2017. PMID: 28434676 Review.
-
Cross-sectional study of male sexual function in bariatric patients.Wideochir Inne Tech Maloinwazyjne. 2016;11(3):171-177. doi: 10.5114/wiitm.2016.62135. Epub 2016 Sep 2. Wideochir Inne Tech Maloinwazyjne. 2016. PMID: 27829940 Free PMC article.
Cited by
-
Influence of Bariatric Surgery on Erectile Dysfunction-a Systematic Review and Meta-Analysis.Obes Surg. 2023 Jun;33(6):1652-1658. doi: 10.1007/s11695-023-06572-9. Epub 2023 Apr 22. Obes Surg. 2023. PMID: 37086370 Free PMC article.
-
Early Effect of Metabolic Surgery on Erectile Function and Ejaculation: a Pilot Study of Obese Men with Type 2 Diabetes Mellitus.Obes Surg. 2020 Dec;30(12):4768-4773. doi: 10.1007/s11695-020-04879-5. Epub 2020 Jul 28. Obes Surg. 2020. PMID: 32725592
-
The Mechanisms and Management of Age-Related Oxidative Stress in Male Hypogonadism Associated with Non-communicable Chronic Disease.Antioxidants (Basel). 2021 Nov 18;10(11):1834. doi: 10.3390/antiox10111834. Antioxidants (Basel). 2021. PMID: 34829704 Free PMC article. Review.
-
The Italian Society of Andrology and Sexual Medicine (SIAMS), along with ten other Italian Scientific Societies, guidelines on the diagnosis and management of erectile dysfunction.J Endocrinol Invest. 2023 Jun;46(6):1241-1274. doi: 10.1007/s40618-023-02015-5. Epub 2023 Jan 25. J Endocrinol Invest. 2023. PMID: 36698034 Free PMC article.
-
Male Obesity Associated Gonadal Dysfunction and the Role of Bariatric Surgery.Front Endocrinol (Lausanne). 2020 Jun 19;11:408. doi: 10.3389/fendo.2020.00408. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32636807 Free PMC article. Review.
References
-
- Adams K.F., Schatzkin A., Harris T.B. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med. 2006;355:763–778. - PubMed
-
- LeBlanc E.S., Patnode C.D., Webber E.M. Behavioral and pharmacotherapy weight loss interventions to prevent obesity-related morbidity and mortality in adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2018;320:1172–1191. - PubMed
-
- Pastuszak A.W., Badhiwala N., Lipshultz L.I. Depression is correlated with the psychological and physical aspects of sexual dysfunction in men. Int J Impot Res. 2013;25:194–199. - PubMed
