

Long-term safety and limited organ damage in patients with systemic lupus erythematosus treated with belimumab: a Phase III study extension
- PMID: 31302695
- PMCID: PMC7571485
- DOI: 10.1093/rheumatology/kez279
Long-term safety and limited organ damage in patients with systemic lupus erythematosus treated with belimumab: a Phase III study extension
Abstract
Objective: This extension study of the Phase III, randomized, placebo-controlled Belimumab International SLE Study (BLISS)-52 and BLISS-76 studies allowed non-US patients with SLE to continue belimumab treatment, in order to evaluate its long-term safety and tolerability including organ damage accrual.
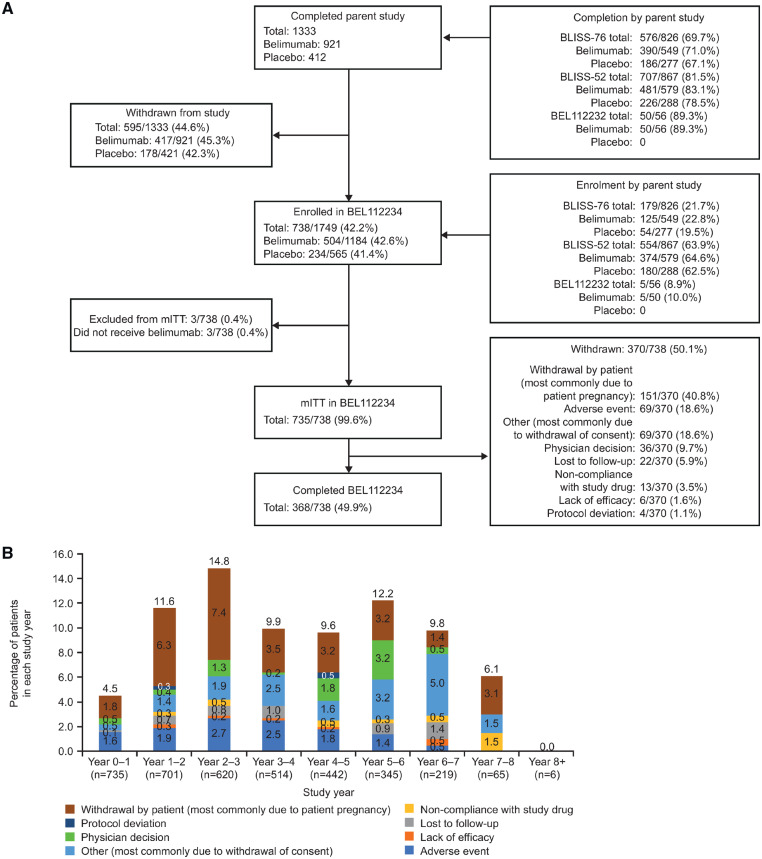
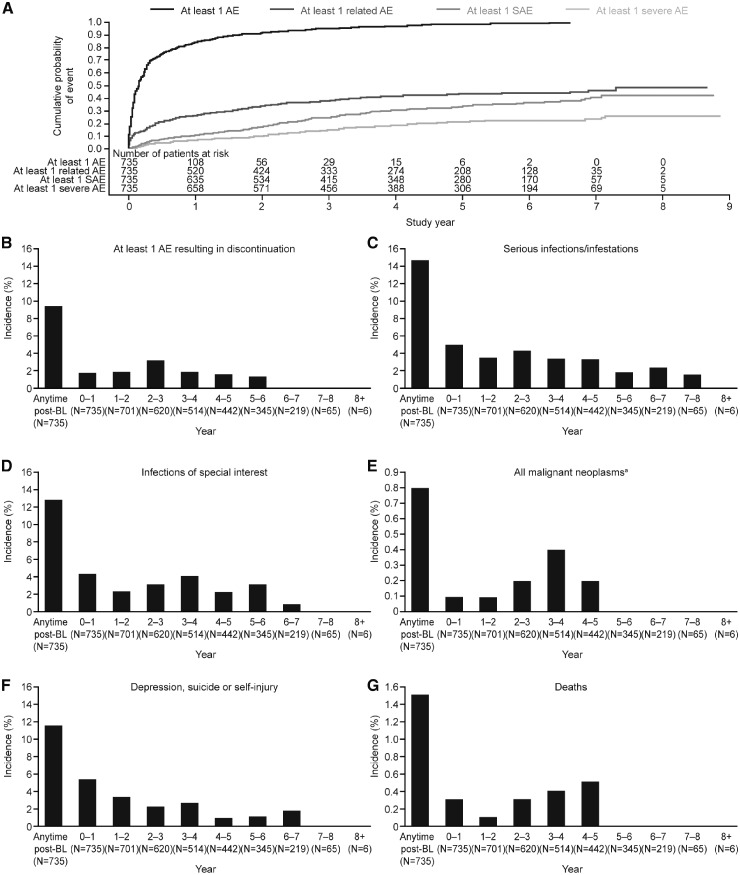
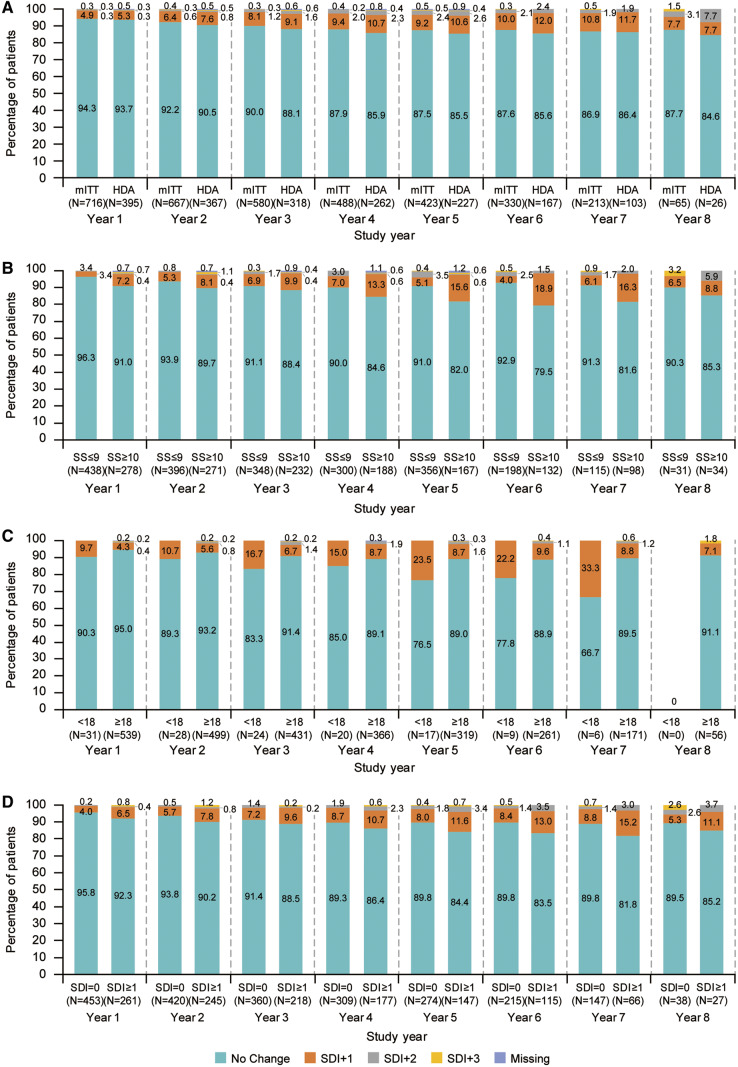
Methods: In this multicentre, long-term extension study (GlaxoSmithKline Study BEL112234) patients received i.v. belimumab every 4 weeks plus standard therapy. Adverse events (AEs) were assessed monthly and safety-associated laboratory parameters were assessed at regular intervals. Organ damage (SLICC/ACR Damage Index) was assessed every 48 weeks. The study continued until belimumab was commercially available, with a subsequent 8-week follow-up period.
Results: A total of 738 patients entered the extension study and 735/738 (99.6%) received one or more doses of belimumab. Annual incidence of AEs, including serious and severe AEs, remained stable or declined over time. Sixty-nine (9.4%) patients experienced an AE resulting in discontinuation of belimumab or withdrawal from the study. Eleven deaths occurred (and two during post-treatment follow-up), including one (cardiogenic shock) considered possibly related to belimumab. Laboratory parameters generally remained stable. The mean (s.d.) SLICC/ACR Damage Index score was 0.6 (1.02) at baseline (prior to the first dose of belimumab) and remained stable. At study year 8, 57/65 (87.7%) patients had no change in SLICC/ACR Damage Index score from baseline, indicating low organ damage accrual.
Conclusion: Belimumab displayed a stable safety profile with no new safety signals. There was minimal organ damage progression over 8 years.
Trial registration: ClinicalTrials.gov, https://clinicaltrials.gov, NCT00424476 (BLISS-52), NCT00410384 (BLISS-76), NCT00732940 (BEL112232), NCT00712933 (BEL112234).
Keywords: belimumab; long-term treatment; organ damage; safety; systemic lupus erythematosus.
© The Author(s) 2019. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures
References
-
- Zhang J, Roschke V, Baker KP. et al. Cutting edge: a role for B lymphocyte stimulator in systemic lupus erythematosus. J Immunol 2001;166:6–10. - PubMed
-
- Arbuckle MR, McClain MT, Rubertone MV. et al. Development of autoantibodies before the clinical onset of systemic lupus erythematosus. N Engl J Med 2003;349:1526–33. - PubMed
-
- Fernandez D, Kirou KA.. What causes lupus flares? Curr Rheumatol Rep 2016;18:14. - PubMed
