

Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis
- PMID: 31303314
- PMCID: PMC6891890
- DOI: 10.1016/S0140-6736(19)31135-3
Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis
Erratum in
-
Department of Error.Lancet. 2019 Sep 14;394(10202):918. doi: 10.1016/S0140-6736(19)31677-0. Lancet. 2019. PMID: 31526735 Free PMC article. No abstract available.
Abstract
Background: Schizophrenia is one of the most common, burdensome, and costly psychiatric disorders in adults worldwide. Antipsychotic drugs are its treatment of choice, but there is controversy about which agent should be used. We aimed to compare and rank antipsychotics by quantifying information from randomised controlled trials.
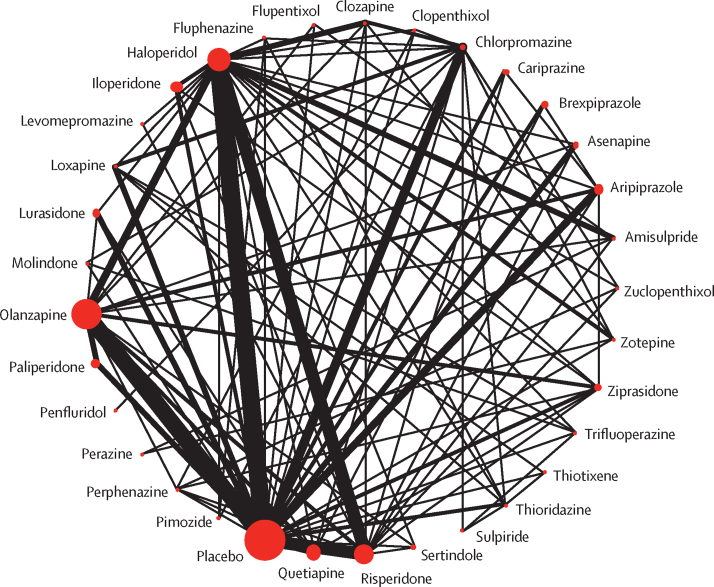
Methods: We did a network meta-analysis of placebo-controlled and head-to-head randomised controlled trials and compared 32 antipsychotics. We searched Embase, MEDLINE, PsycINFO, PubMed, BIOSIS, Cochrane Central Register of Controlled Trials (CENTRAL), WHO International Clinical Trials Registry Platform, and ClinicalTrials.gov from database inception to Jan 8, 2019. Two authors independently selected studies and extracted data. We included randomised controlled trials in adults with acute symptoms of schizophrenia or related disorders. We excluded studies in patients with treatment resistance, first episode, predominant negative or depressive symptoms, concomitant medical illnesses, and relapse-prevention studies. Our primary outcome was change in overall symptoms measured with standardised rating scales. We also extracted data for eight efficacy and eight safety outcomes. Differences in the findings of the studies were explored in metaregressions and sensitivity analyses. Effect size measures were standardised mean differences, mean differences, or risk ratios with 95% credible intervals (CrIs). Confidence in the evidence was assessed using CINeMA (Confidence in Network Meta-Analysis). The study protocol is registered with PROSPERO, number CRD42014014919.
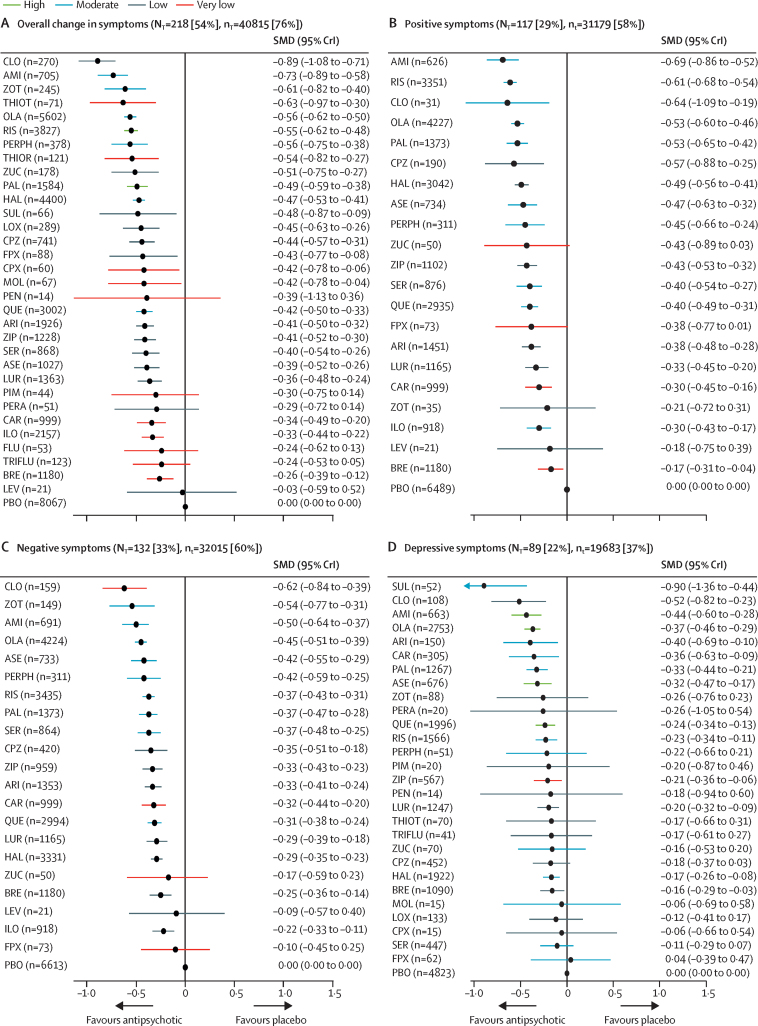
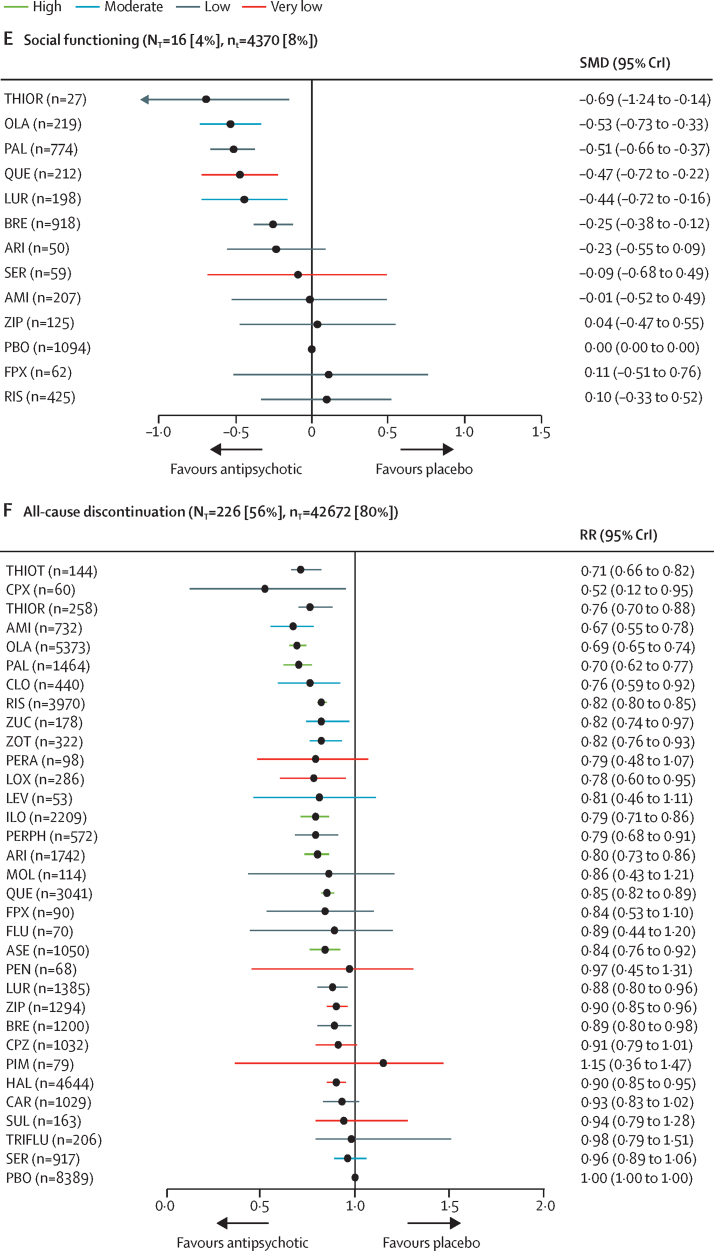
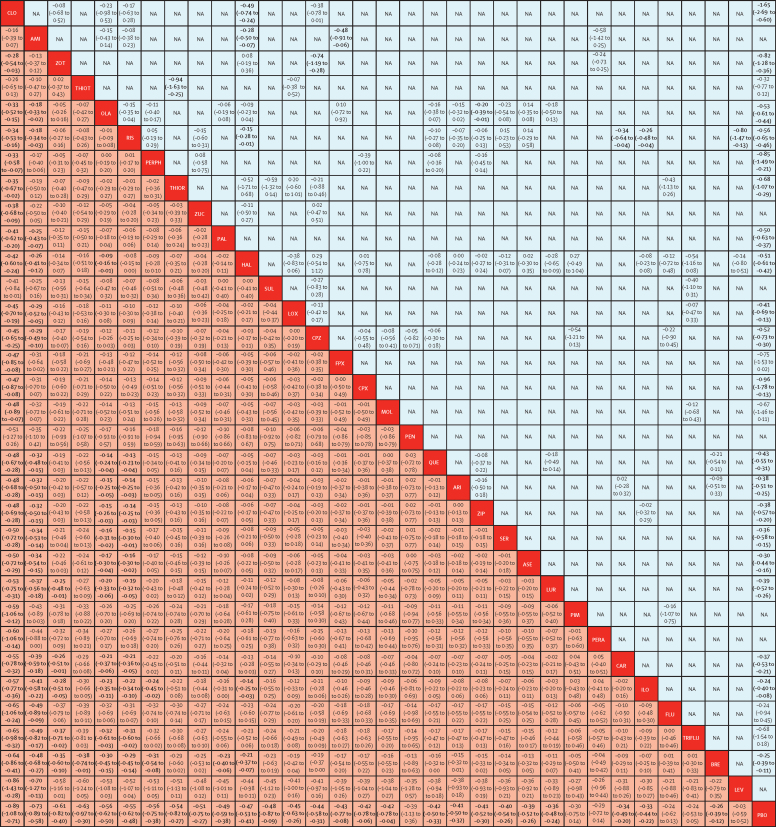
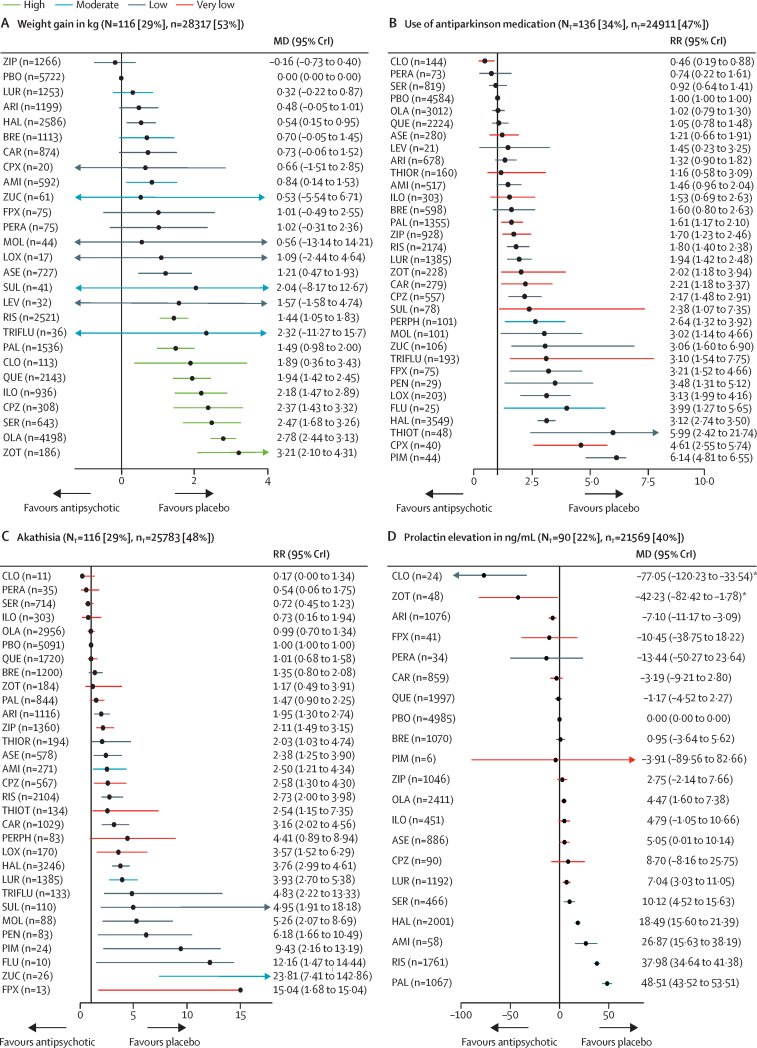
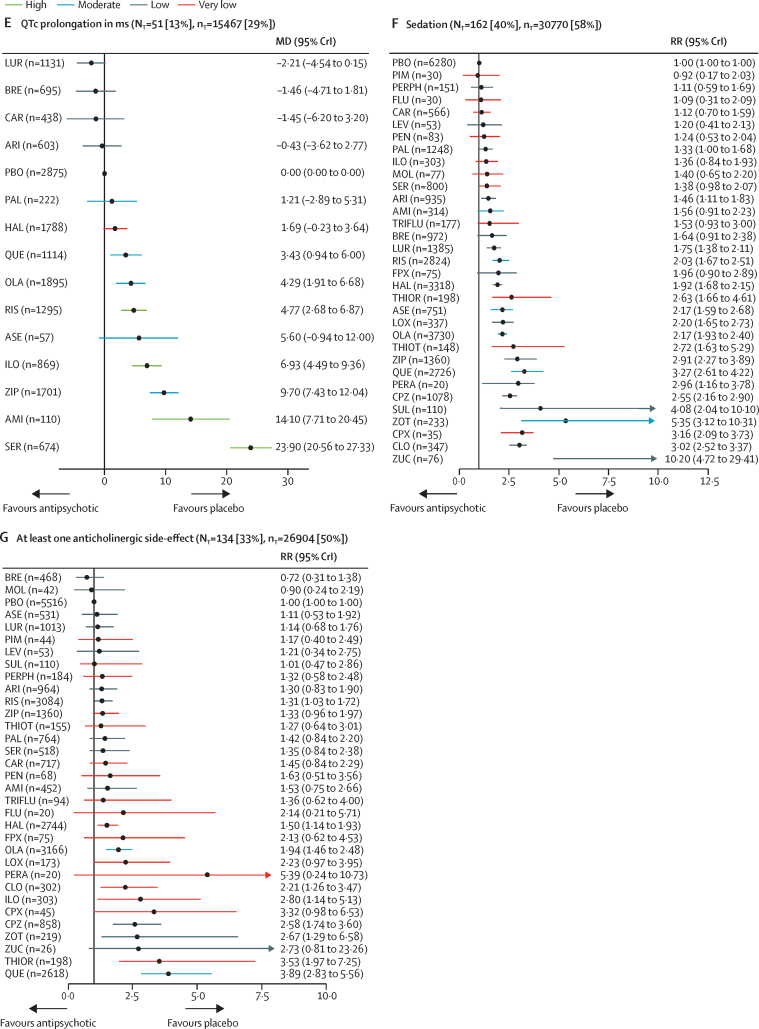
Findings: We identified 54 417 citations and included 402 studies with data for 53 463 participants. Effect size estimates suggested all antipsychotics reduced overall symptoms more than placebo (although not statistically significant for six drugs), with standardised mean differences ranging from -0·89 (95% CrI -1·08 to -0·71) for clozapine to -0·03 (-0·59 to 0·52) for levomepromazine (40 815 participants). Standardised mean differences compared with placebo for reduction of positive symptoms (31 179 participants) varied from -0·69 (95% CrI -0·86 to -0·52) for amisulpride to -0·17 (-0·31 to -0·04) for brexpiprazole, for negative symptoms (32 015 participants) from -0·62 (-0·84 to -0·39; clozapine) to -0·10 (-0·45 to 0·25; flupentixol), for depressive symptoms (19 683 participants) from -0·90 (-1·36 to -0·44; sulpiride) to 0·04 (-0·39 to 0·47; flupentixol). Risk ratios compared with placebo for all-cause discontinuation (42 672 participants) ranged from 0·52 (0·12 to 0·95; clopenthixol) to 1·15 (0·36 to 1·47; pimozide), for sedation (30 770 participants) from 0·92 (0·17 to 2·03; pimozide) to 10·20 (4·72 to 29·41; zuclopenthixol), for use of antiparkinson medication (24 911 participants) from 0·46 (0·19 to 0·88; clozapine) to 6·14 (4·81 to 6·55; pimozide). Mean differences compared to placebo for weight gain (28 317 participants) ranged from -0·16 kg (-0·73 to 0·40; ziprasidone) to 3·21 kg (2·10 to 4·31; zotepine), for prolactin elevation (21 569 participants) from -77·05 ng/mL (-120·23 to -33·54; clozapine) to 48·51 ng/mL (43·52 to 53·51; paliperidone) and for QTc prolongation (15 467 participants) from -2·21 ms (-4·54 to 0·15; lurasidone) to 23·90 ms (20·56 to 27·33; sertindole). Conclusions for the primary outcome did not substantially change after adjusting for possible effect moderators or in sensitivity analyses (eg, when excluding placebo-controlled studies). The confidence in evidence was often low or very low.
Interpretation: There are some efficacy differences between antipsychotics, but most of them are gradual rather than discrete. Differences in side-effects are more marked. These findings will aid clinicians in balancing risks versus benefits of those drugs available in their countries. They should consider the importance of each outcome, the patients' medical problems, and preferences.
Funding: German Ministry of Education and Research and National Institute for Health Research.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Balancing body and mind: selecting the optimal antipsychotic.Lancet. 2019 Sep 14;394(10202):900-902. doi: 10.1016/S0140-6736(19)32096-3. Lancet. 2019. PMID: 31526722 No abstract available.
-
Review: In multiepisode schizophrenia, most antipsychotic drugs improve symptoms; adverse effects vary by drug.Ann Intern Med. 2019 Nov 19;171(10):JC57. doi: 10.7326/ACPJ201911190-057. Ann Intern Med. 2019. PMID: 31739340 No abstract available.
-
Antipsychotics for schizophrenia and substance misuse.Lancet. 2020 Jun 20;395(10241):1902. doi: 10.1016/S0140-6736(20)30237-3. Lancet. 2020. PMID: 32563367 No abstract available.
-
Preventing relapse in schizophrenia needs better evidence.Lancet. 2022 Feb 26;399(10327):773-775. doi: 10.1016/S0140-6736(21)02142-5. Lancet. 2022. PMID: 35219386 No abstract available.
References
-
- Cloutier M, Aigbogun MS, Guerin A. The economic burden of schizophrenia in the United States in 2013. J Clin Psychiatry. 2016;77:764–771. - PubMed
-
- Leucht S, Cipriani A, Spineli L. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. 2013;382:951–962. - PubMed
-
- Oehl M, Hummer M, Fleischhacker WW. Compliance with antipsychotic treatment. Acta Psychiatr Scand. 2000;102:83–86. - PubMed
-
- WHO Collaborating Centre for Drug Statistics Methodology . WHO Collaborating Centre for Drug Statistics Methodology; 2018. ATC/DDD Index—antipsychotics.https://www.whocc.no/atc_ddd_index/?code=N05A
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
