

Postoperative opioid prescribing is not my job: A qualitative analysis of care transitions
- PMID: 31303324
- PMCID: PMC7068723
- DOI: 10.1016/j.surg.2019.05.033
Postoperative opioid prescribing is not my job: A qualitative analysis of care transitions
Abstract
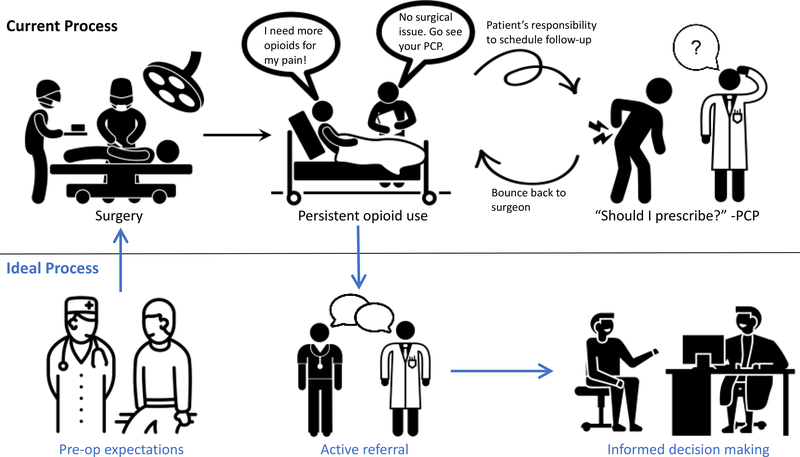
Background: Persistent opioid use is common after surgical procedures, and postoperative opioid prescribing often transitions from surgeons to primary care physicians in the months after surgery. It is unknown how surgeons currently transition these patients or the preferred approach to successful coordination of care. This qualitative study aimed to describe transitions of care for postoperative opioid prescribing and identify barriers and facilitators of ideal transitions for potential intervention targets.
Methods: We conducted a qualitative study of surgeons and primary care physicians at a large academic healthcare system using a semi-structured interview guide. Transcripts were independently coded using the Theoretical Domains Framework to identify underlying determinants of physician behaviors. We mapped dominant themes to the Behavior Change Wheel to propose potential interventions targeting these behaiors.
Results: Physicians were interviewed between July 2017 and December 2017 beyond thematic saturation (n = 20). Surgeons report passive transitions to primary care physicians after ruling out surgical complications, and these patients often bounce back to the surgeon when primary care physicians are uncertain of the cause of ongoing pain. Ideal practices were identified as setting preoperative expectations and engaging in active transition for postoperative opioid prescribing. We identified 3 behavioral targets for multidisciplinary intervention: knowledge (guidelines for coordination of care), barriers (utilizing support staff for active transition), and professional role (incentive for multidisciplinary collaboration).
Conclusion: This qualitative study identifies potential interventions aimed at changing physician behaviors regarding transitions of care for postoperative opioid prescribing. Implementation of these interventions could improve coordination of care for patients with persistent postoperative opioid use.
Copyright © 2019. Published by Elsevier Inc.
Figures


References
-
- Soneji N, Clarke HA, Ko DT, Wijeysundera DN. Risks of Developing Persistent Opioid Use After Major Surgery. JAMA Surg. 2016;151(11):1083–1084. - PubMed
-
- Alam A, Gomes T, Zheng H, Mamdani MM, Juurlink DN, Bell CM. Long-term analgesic use after low-risk surgery: a retrospective cohort study. Arch Intern Med. 2012;172(5):425–430. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
