

Long-term health outcomes and cost-effectiveness of coronary CT angiography in patients with suspicion for acute coronary syndrome
- PMID: 31303580
- PMCID: PMC6930365
- DOI: 10.1016/j.jcct.2019.06.008
Long-term health outcomes and cost-effectiveness of coronary CT angiography in patients with suspicion for acute coronary syndrome
Abstract
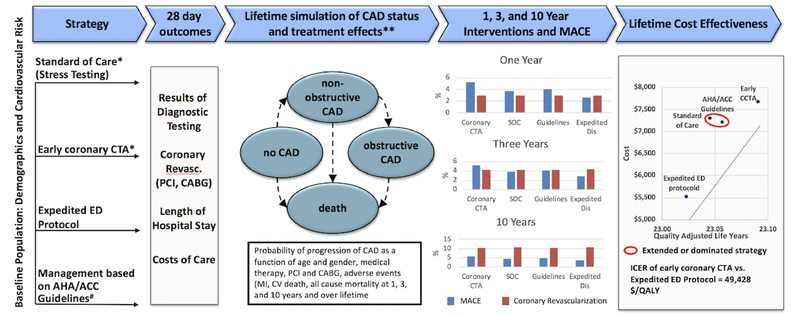
Background: Randomized trials have shown favorable clinical outcomes for coronary CT angiography (CTA) in patients with suspected acute coronary syndrome (ACS). Our goal was to estimate the cost-effectiveness of coronary CTA as compared to alternative management strategies for ACP patients over lifetime.
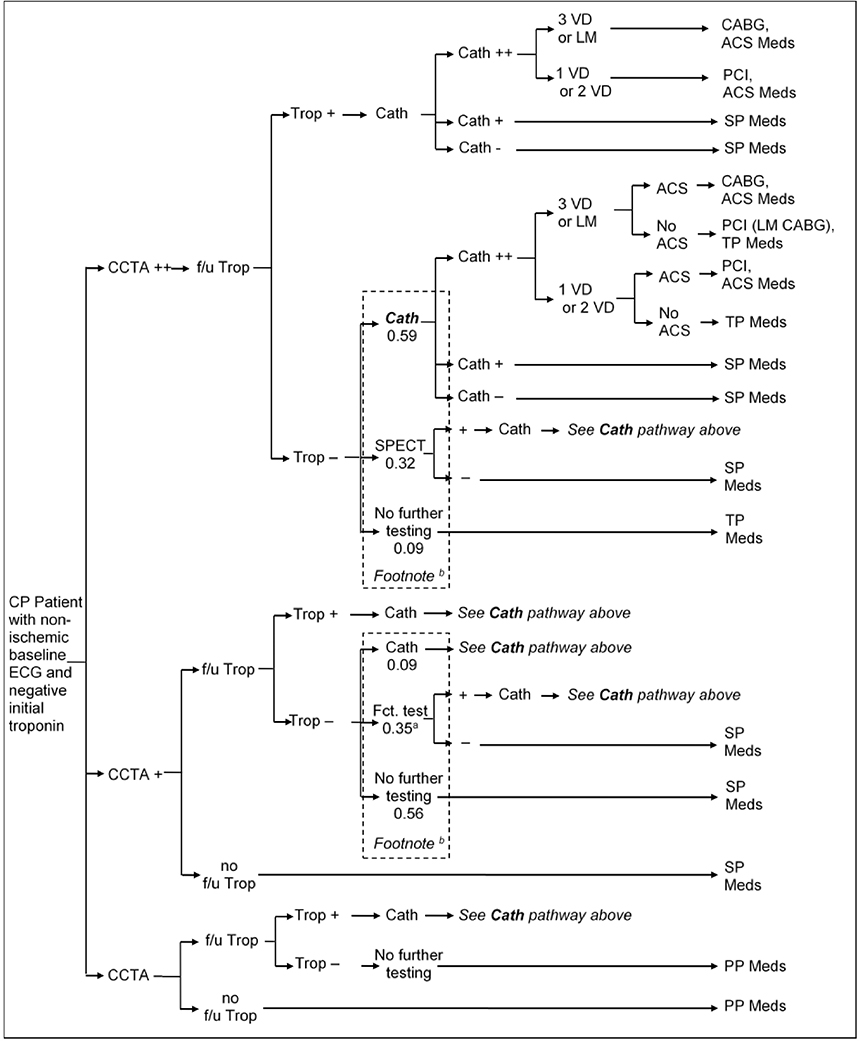
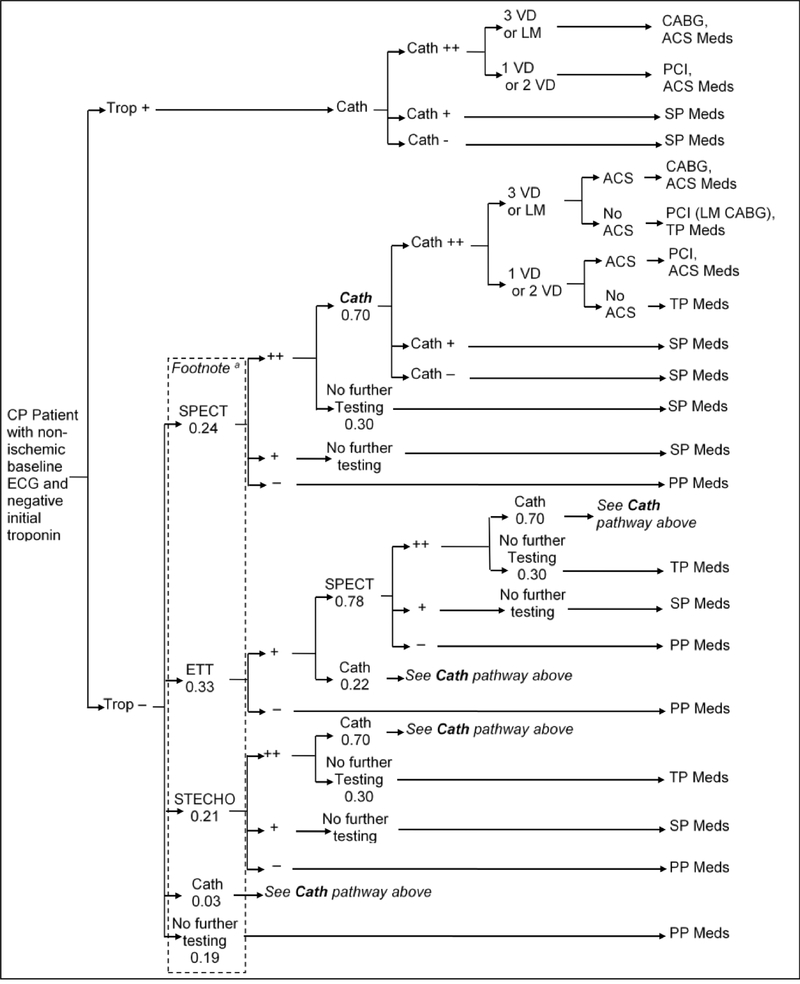
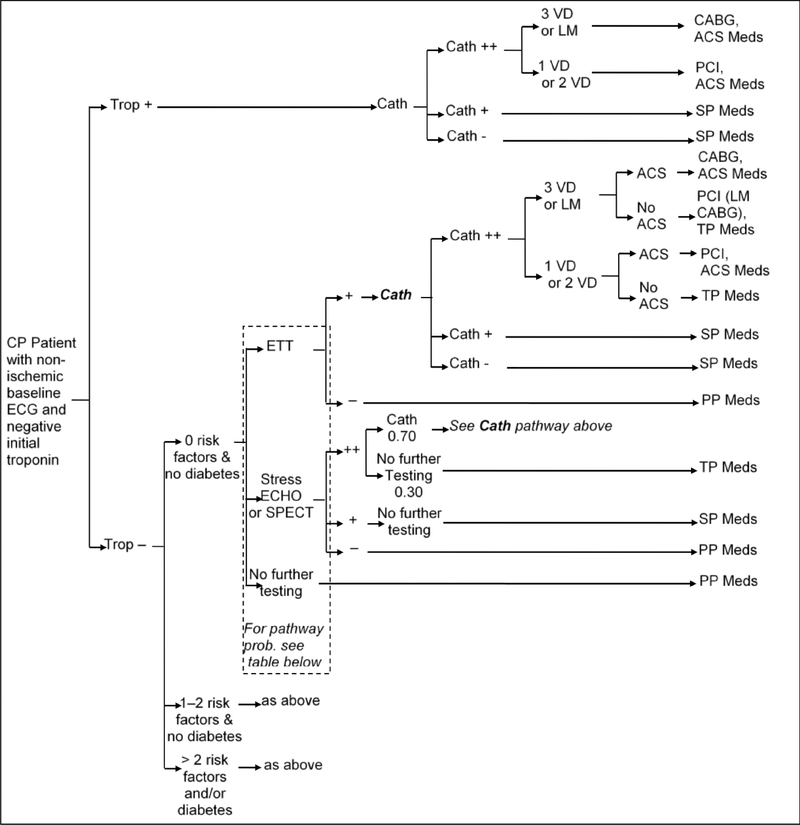
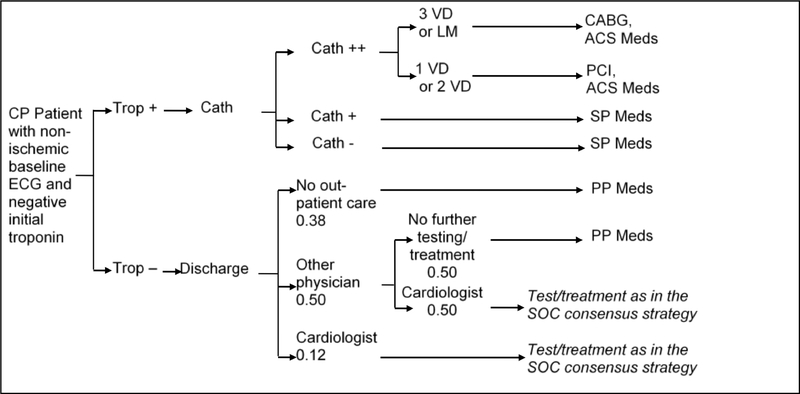
Methods: Markov microsimulation model was developed to compare cost-effectiveness of competitive strategies for ACP patients: 1) coronary CTA, 2) standard of care (SOC), 3) AHA/ACC Guidelines, and 4) expedited emergency department (ED) discharge protocol with outpatient testing. ROMICAT-II trial was used to populate the model with low to intermediate risk of ACS patient data, whereas diagnostic test-, treatment effect-, morbidity/mortality-, quality of life- and cost data were obtained from the literature. We predicted test utilization, costs, 1-, 3-, 10-year and over lifetime cardiovascular morbidity/mortality for each strategy. We determined quality adjusted life years (QALY) and incremental cost-effectiveness ratio. Observed outcomes in ROMICAT-II were used to validate the short-term model.
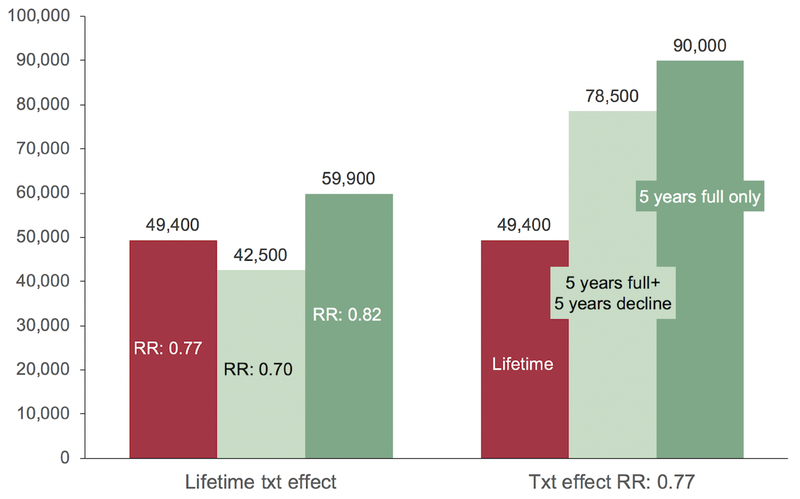
Results: Estimated short-term outcomes accurately reflected observed outcomes in ROMICAT-II as coronary CTA was associated with higher costs ($4,490 vs. $2,513-$4,144) and revascularization rates (5.2% vs. 2.6%-3.7%) compared to alternative strategies. Over lifetime, coronary CTA dominated SOC and ACC/AHA Guidelines and was cost-effective compared to expedited ED protocol ($49,428/QALY). This was driven by lower cardiovascular mortality (coronary CTA vs. expedited discharge: 3-year: 1.04% vs. 1.10-1.17; 10-year: 5.06% vs. 5.21-5.36%; respectively).
Conclusion: Coronary CTA in patients with suspected ACS renders affordable long-term health benefits as compared to alternative strategies.
Keywords: Acute chest pain; Acute coronary syndrome; Coronary CTA; Cost-effectiveness analysis; Markov microsimulation model.
Copyright © 2020 Society of Cardiovascular Computed Tomography. All rights reserved.
Figures
References
-
- Litt HI, Gatsonis C, Snyder B, Singh H, Miller CD, Entrikin DW, Leaming JM, Gavin LJ, Pacella CB and Hollander JE. CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med. 2012;366:1393–403. - PubMed
-
- Hoffmann U, Truong QA, Schoenfeld DA, Chou ET, Woodard PK, Nagurney JT, Pope JH, Hauser TH, White CS, Weiner SG, Kalanjian S, Mullins ME, Mikati I, Peacock WF, Zakroysky P, Hayden D, Goehler A, Lee H, Gazelle GS, Wiviott SD, Fleg JL, Udelson JE and Investigators R-I. Coronary CT angiography versus standard evaluation in acute chest pain. N Engl J Med. 2012;367:299–308. - PMC - PubMed
-
- Goldstein JA, Chinnaiyan KM, Abidov A, Achenbach S, Berman DS, Hayes SW, Hoffmann U, Lesser JR, Mikati IA, O’Neil BJ, Shaw LJ, Shen MY, Valeti US and Raff GL. The CT-STAT (Coronary Computed Tomographic Angiography for Systematic Triage of Acute Chest Pain Patients to Treatment) trial. J Am Coll Cardiol. 2011;58:1414–22. - PubMed
-
- Schlett CL, Banerji D, Siegel E, Bamberg F, Lehman SJ, Ferencik M, Brady TJ, Nagurney JT, Hoffmann U and Truong QA. Prognostic value of CT angiography for major adverse cardiac events in patients with acute chest pain from the emergency department: 2-year outcomes of the ROMICAT trial. JACC Cardiovasc Imaging. 2011;4:481–491. - PMC - PubMed
-
- Jones RL, Thomas DM, Barnwell ML, Fentanes E, Young AN, Barnwell R, Foley AT, Hilliard M, Hulten EA, Villines TC, Cury RC and Slim AM. Safe and rapid disposition of low-to-intermediate risk patients presenting to the emergency department with chest pain: a 1-year high-volume single-center experience. J Cardiovasc Comput Tomogr. 2014;8:375–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
