

Evaluation of patients submitted to the arthroscopic treatment of the lateral epicondylitis refractory to the conservative treatment
- PMID: 31304165
- PMCID: PMC6565965
- DOI: 10.1016/j.rboe.2013.12.018
Evaluation of patients submitted to the arthroscopic treatment of the lateral epicondylitis refractory to the conservative treatment
Abstract
Objective: to evaluate the results of the arthroscopic treatment of the lateral epicondylitis.
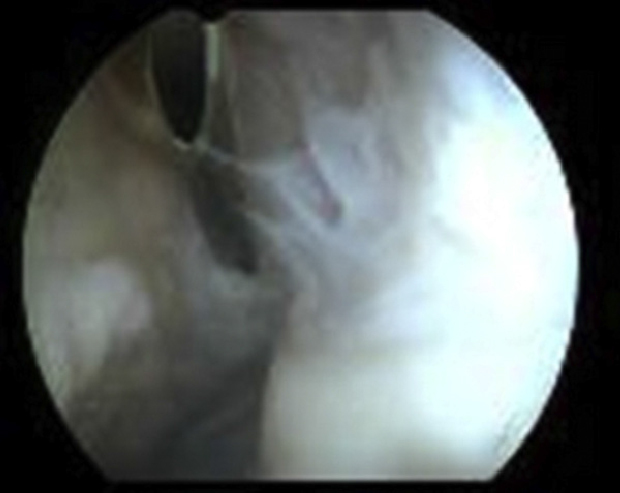
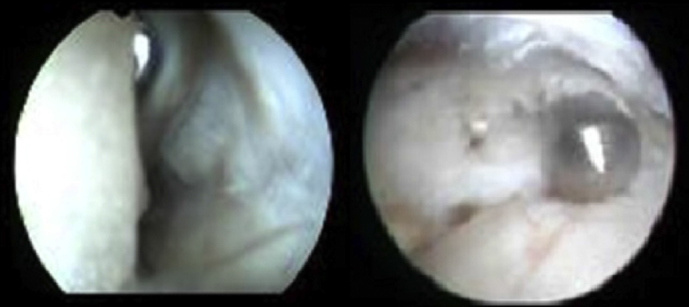
Methods: we evaluated 14 patients (15 elbows) submitted to the arthroscopic treatment of the lateral epicondylitis refractory to the conservative treatment, which was realized for a minimum period of 18 months. Beyond the demographic data collection, patients were evaluated according to the arthroscopic classification of Baker et al., the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire and the Mayo Elbow Performance Score (MEPS). The patients' ages ranged between 23 and 56 years (average 46 years) (eight males and six females). Of the 15 elbows, 12 were the dominant and one patient had bilateral lesion. The follow-up after surgery was minimum 24 months and maximum 72 months (average 41 months).
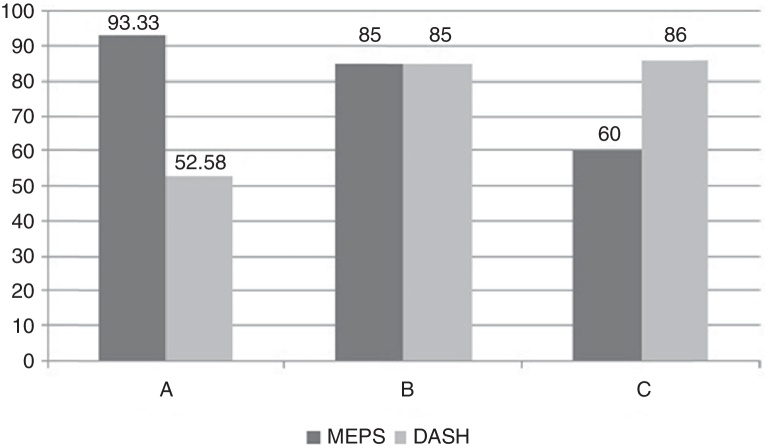
Results: we found, according to the arthroscopic classification of Baker et al., two patients with type I lesions, nine with type II lesions and three with type III lesions. We found the following complications: one patient with altered sensitivity in the region of the lateral portal, one with a deficit of ten degrees in length, one with synovial plica and one with synovitis in the lateral compartment. Our score on the DASH questionnaire was minimum of 32 points and maximum of 120 points (average 57 points) and the scale of MEPS had a minimum score of 60 points and a maximum of 100 points (average 90 points).
Conclusion: the arthroscopic treatment of the lateral epicondylitis, plus insurance, provides satisfactory results.
Objetivo: avaliar os resultados do tratamento artroscópico da epicondilite lateral.
Métodos: foram avaliados 14 pacientes (15 cotovelos) submetidos ao tratamento artroscópico da epicondilite lateral refratária ao tratamento conservador, o qual foi feito por um período mínimo de 18 meses. Além da coleta de dados demográficos, os pacientes foram avaliados segundo a classificação artroscópica de Baker et al., o questionário Disabilities of the Arm, Shoulder, and Hand (DASH) e o Mayo Elbow Performance Score (MEPS). As idades dos pacientes variaram entre 23 e 56 anos (média de 46) e foram oito do sexo masculino e seis do feminino. Dos 15 cotovelos, 12 eram do membro dominante e um paciente tinha lesão bilateral. O seguimento após a cirurgia foi de no mínimo 24 meses e no máximo 72 meses (média de 41).
Resultados: foram constatadas, segundo a classificação artroscópica de Baker et al., dois pacientes com lesão do tipo I, nove com lesão do tipo II e três com lesão do tipo III. Encontramos as seguintes complicações: um paciente com alteração da sensibilidade na região do portal lateral, um com déficit de dez graus na extensão, um com plica sinovial e um com sinovite em compartimento lateral. Nossa pontuação no questionário DASH foi de no mínimo 32 pontos e no máximo 120 pontos (média de 57) e a escala de MEPS apresentou pontuação mínima de 60 pontos e máxima de 100 pontos (média de 90 pontos).
Conclusão: o tratamento artroscópico da epicondilite lateral, além de seguro, apresenta resultados satisfatórios.
Keywords: Arthroscopy; Tennis elbow/complications; Tennis elbow/surgery; Tennis elbow/therapy.
Figures
Similar articles
-
Functional outcomes after arthroscopic treatment of lateral epicondylitis.J Orthop Sci. 2009 Mar;14(2):167-74. doi: 10.1007/s00776-008-1304-9. Epub 2009 Apr 1. J Orthop Sci. 2009. PMID: 19337808
-
A randomized, double-blind sham-controlled trial on the efficacy of arthroscopic tennis elbow release for the management of chronic lateral epicondylitis.BMC Musculoskelet Disord. 2016 Jun 1;17:239. doi: 10.1186/s12891-016-1093-9. BMC Musculoskelet Disord. 2016. PMID: 27245219 Free PMC article. Clinical Trial.
-
Modified arthroscopic tenotomy of the extensor carpi radialis brevis for refractory lateral epicondylitis: a cohort study.J Shoulder Elbow Surg. 2024 Mar;33(3):536-543. doi: 10.1016/j.jse.2023.09.036. Epub 2023 Nov 7. J Shoulder Elbow Surg. 2024. PMID: 37944746
-
Comparison of Clinical Outcomes After Different Surgical Approaches for Lateral Epicondylitis: A Systematic Review and Meta-analysis.Orthop J Sports Med. 2024 May 2;12(5):23259671241230291. doi: 10.1177/23259671241230291. eCollection 2024 May. Orthop J Sports Med. 2024. PMID: 38708009 Free PMC article. Review.
-
Heterotopic Ossification After the Arthroscopic Treatment of Lateral Epicondylitis.Hand (N Y). 2017 May;12(3):NP32-NP36. doi: 10.1177/1558944716668844. Hand (N Y). 2017. PMID: 28453354 Free PMC article. Review.
Cited by
-
Is There any Difference in Clinical Outcome between Open and Arthroscopic Treatment for Tennis Elbow? A Systematic Review and Meta-Analysis.Orthop Surg. 2023 Aug;15(8):1931-1943. doi: 10.1111/os.13570. Epub 2022 Nov 29. Orthop Surg. 2023. PMID: 36444948 Free PMC article.
-
Arthroscopic surgical treatment of recalcitrant lateral epicondylitis - A series of 47 cases.Rev Bras Ortop. 2016 Dec 21;52(1):46-51. doi: 10.1016/j.rboe.2016.03.008. eCollection 2017 Jan-Feb. Rev Bras Ortop. 2016. PMID: 28194381 Free PMC article.
References
-
- Johnson G.W., Cadwallader K., Scheffel S.B., Epperly T.D. Treatment of lateral epicondylitis. Am Fam Physician. 2007;76(6):843–848. - PubMed
-
- Savoie F.H., VanSice W., O’Brien M.J. Arthroscopic tennis elbow release. J Shoulder Elbow Surg. 2010;19(2):31–36. - PubMed
-
- Baker C.L., Baker C.L., 3rd Long-term follow-up of arthroscopic treatment of lateral epicondylitis. Am J Sports Med. 2008;36(2):254–260. - PubMed
-
- Kim J.W., Chun C.H., Shim D.M., Kim T.K., Kweon S.H., Kang H.J. Arthroscopic treatment of lateral epiconsylitis: comparison of the outcome of ECRB release with an without decortication. Knee Surg Sports Traumatol Arthrosc. 2011;19(7):1178–1183. - PubMed
-
- Lattermann C., Romeo A.A., Anbari A., Meininger K., McCarty L.P., Cole B.J. Arthroscopic debridement of the extensor carpi radialis brevis for recalcitrant lateral epicondylitis. J Shoulder Elbow Surg. 2010;19(5):651–656. - PubMed
LinkOut - more resources
Full Text Sources