

Smartphone-based migraine behavioral therapy: a single-arm study with assessment of mental health predictors
- PMID: 31304392
- PMCID: PMC6550263
- DOI: 10.1038/s41746-019-0116-y
Smartphone-based migraine behavioral therapy: a single-arm study with assessment of mental health predictors
Abstract
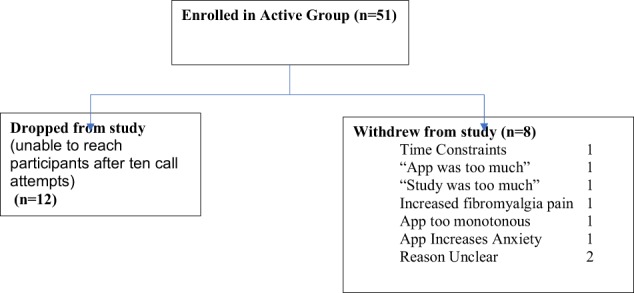
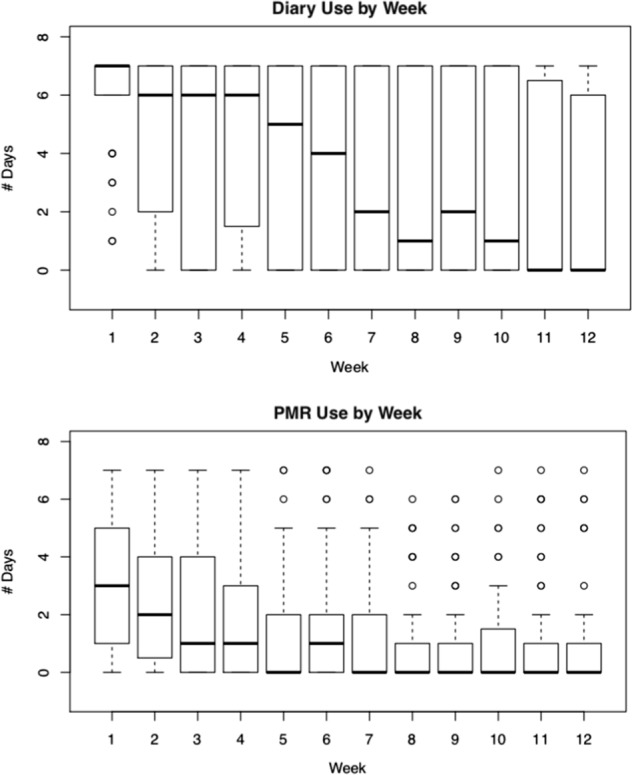
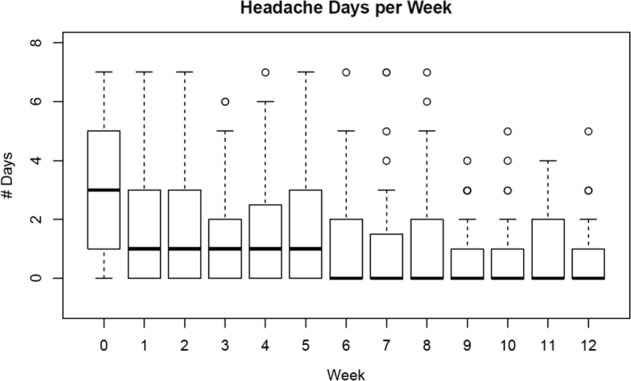
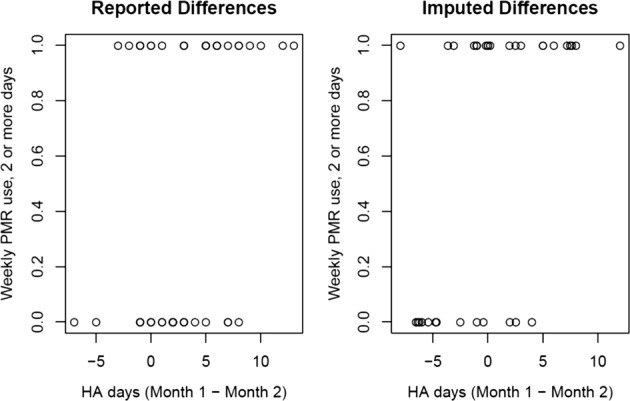
Progressive muscle relaxation (PMR) is an under-utilized Level A evidence-based treatment for migraine prevention. We studied the feasibility and acceptability of smartphone application (app)-based PMR for migraine in a neurology setting, explored whether app-based PMR might reduce headache (HA) days, and examined potential predictors of app and/or PMR use. In this single-arm pilot study, adults with ICHD3 migraine, 4+ HA days/month, a smartphone, and no prior behavioral migraine therapy in the past year were asked to complete a daily HA diary and do PMR for 20 min/day for 90 days. Outcomes were: adherence to PMR (no. and duration of audio plays) and frequency of diary use. Predictors in the models were baseline demographics, HA-specific variables, baseline PROMIS (patient-reported outcomes measurement information system) depression and anxiety scores, presence of overlapping pain conditions studied and app satisfaction scores at time of enrollment. Fifty-one patients enrolled (94% female). Mean age was 39 ± 13 years. The majority (63%) had severe migraine disability at baseline (MIDAS). PMR was played 22 ± 21 days on average. Mean/session duration was 11 ± 7 min. About half (47%) of uses were 1+ time/week and 35% of uses were 2+ times/week. There was a decline in use/week. On average, high users (PMR 2+ days/week in the first month) had 4 fewer days of reported HAs in month 2 vs. month 1, whereas low PMR users (PMR < 2 days/week in the first month) had only 2 fewer HA days in month 2. PROMIS depression score was negatively associated with the log odds of using the diary at least once (vs. no activity) in a week (OR = 0.70, 95% CI = [0.55, 0.85]) and of doing the PMR at least once in a week (OR = 0.77, 95% CI = [0.68, 0.91]). PROMIS anxiety was positively associated with using the diary at least once every week (OR = 1.33, 95% CI = [1.09, 1.73]) and with doing the PMR at least once every week (OR = 1.14 [95% CI = [1.02, 1.31]). In conclusion, about half of participants used smartphone-based PMR intervention based upon a brief, initial introduction to the app. App use was associated with reduction in HA days. Higher depression scores were negatively associated with diary and PMR use, whereas higher anxiety scores were positively associated.
Keywords: Medical research; Neurology.
Conflict of interest statement
Competing interestsThe authors declare both financial and non-financial disclosures, however, none that affect the presented study.
Figures
Similar articles
-
Smartphone based behavioral therapy for pain in multiple sclerosis (MS) patients: A feasibility acceptability randomized controlled study for the treatment of comorbid migraine and ms pain.Mult Scler Relat Disord. 2020 Nov;46:102489. doi: 10.1016/j.msard.2020.102489. Epub 2020 Sep 8. Mult Scler Relat Disord. 2020. PMID: 32950893 Free PMC article. Clinical Trial.
-
Smartphone-Delivered Progressive Muscle Relaxation for the Treatment of Migraine in Primary Care: A Randomized Controlled Trial.Headache. 2020 Nov;60(10):2232-2246. doi: 10.1111/head.14010. Epub 2020 Nov 16. Headache. 2020. PMID: 33200413 Free PMC article. Clinical Trial.
-
Introduction of a smartphone based behavioral intervention for migraine in the emergency department.Gen Hosp Psychiatry. 2021 Mar-Apr;69:12-19. doi: 10.1016/j.genhosppsych.2020.12.009. Epub 2021 Jan 8. Gen Hosp Psychiatry. 2021. PMID: 33485090 Free PMC article.
-
Adherence to Behavioral Therapy for Migraine: Knowledge to Date, Mechanisms for Assessing Adherence, and Methods for Improving Adherence.Curr Pain Headache Rep. 2019 Jan 19;23(1):3. doi: 10.1007/s11916-019-0739-3. Curr Pain Headache Rep. 2019. PMID: 30661135 Free PMC article. Review.
-
Novel Augmentation Strategies in Major Depression.Dan Med J. 2017 Apr;64(4):B5338. Dan Med J. 2017. PMID: 28385173 Review.
Cited by
-
21st century headache: mapping new territory.J Headache Pain. 2021 Apr 1;22(1):19. doi: 10.1186/s10194-021-01233-7. J Headache Pain. 2021. PMID: 33794761 Free PMC article.
-
Computerized migraine diagnostic tools: a systematic review.Ther Adv Chronic Dis. 2022 Jan 24;13:20406223211065235. doi: 10.1177/20406223211065235. eCollection 2022. Ther Adv Chronic Dis. 2022. PMID: 35096362 Free PMC article.
-
Behavioral Therapy Preferences in People With Migraine.Headache. 2020 Jun;60(6):1093-1102. doi: 10.1111/head.13790. Epub 2020 Mar 23. Headache. 2020. PMID: 32207148 Free PMC article.
-
Cognitive Behavioral Therapy for Children With Headaches: Will an App Do the Trick?J Child Neurol. 2023 Mar;38(3-4):169-177. doi: 10.1177/08830738231170067. Epub 2023 Apr 25. J Child Neurol. 2023. PMID: 37097885 Free PMC article. Clinical Trial.
-
Engagement in Digital Self-management Interventions for Chronic Pain: A Systematic Review.Clin J Pain. 2025 Jun 1;41(6):e1289. doi: 10.1097/AJP.0000000000001289. Clin J Pain. 2025. PMID: 40145149
References
-
- Campbell J., Penzien D., Wall E. Evidence-based guidelines for migraine headache: behavioral and physical treatments (Physiotherapy Evidence Database, 2000).
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
