

A Single-Center Experience on Outcomes of Complementary and Alternative Medicine Use Among Patients With Cirrhosis
- PMID: 31304453
- PMCID: PMC6601323
- DOI: 10.1002/hep4.1355
A Single-Center Experience on Outcomes of Complementary and Alternative Medicine Use Among Patients With Cirrhosis
Abstract
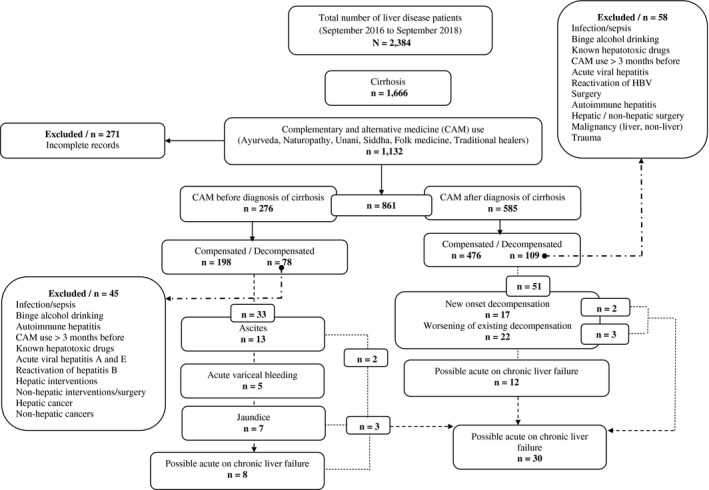
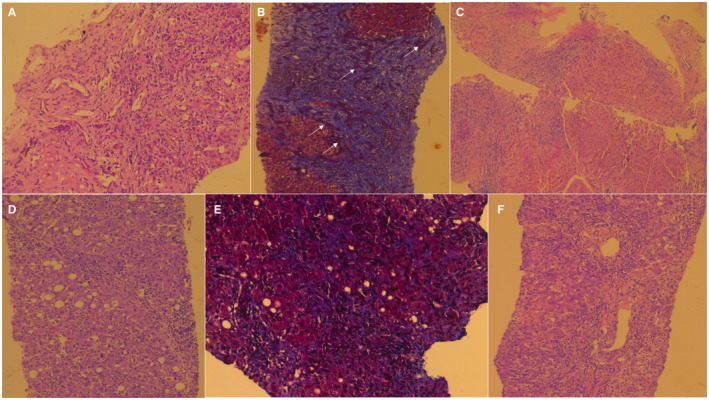
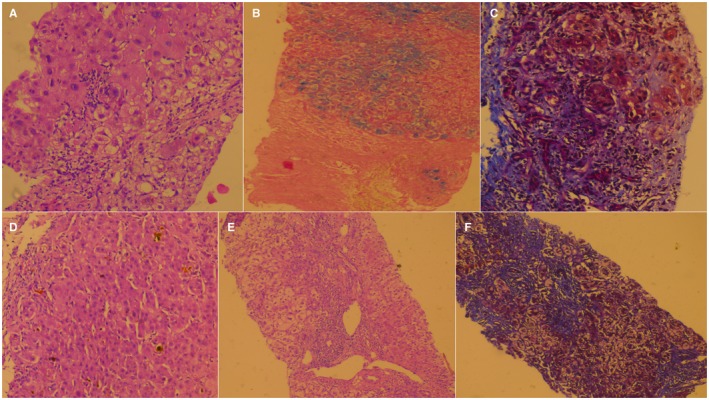
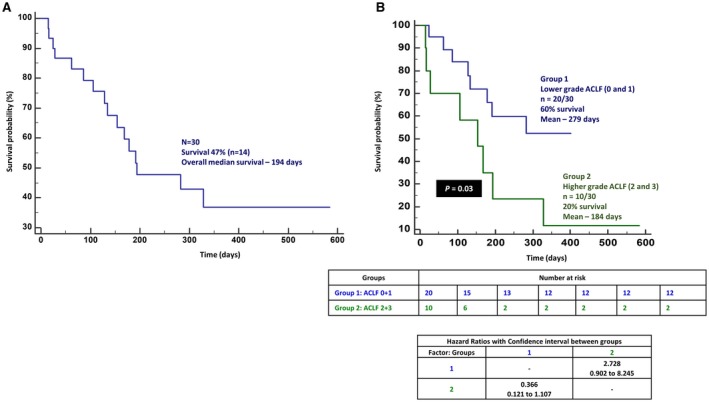
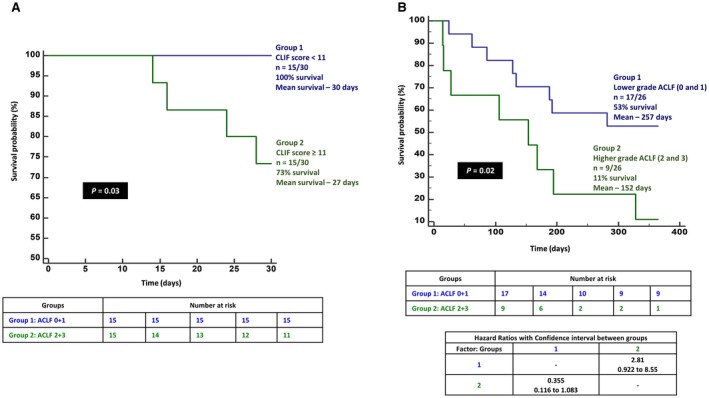
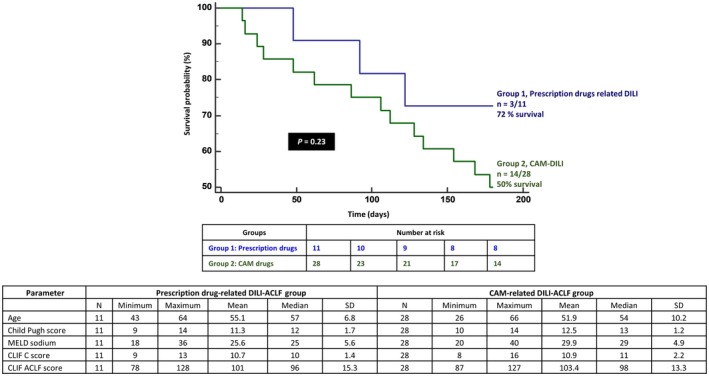
Drug-induced liver injury (DILI) due to complementary and alternative medicine (CAM) use is on the rise throughout the world by patients looking for "safer" alternatives. However, data on acute-on-chronic liver failure (ACLF) due to CAM are lacking. In a large cohort of patients with cirrhosis, we retrospectively studied CAM-related health-seeking behavior and attempted to identify those who developed possible CAM-DILI-related ACLF. In this study, we examine the clinical, biochemical, and liver histopathologic characteristics of possible CAM-DILI-related ACLF, describe implicated CAM agents, and discuss predictors of patient outcomes. Out of 1,666 patients with cirrhosis, 68% used CAM at some point. A total of 35.7% (n = 30/84) patients presented with CAM-related DILI leading to ACLF in the whole CAM-DILI-related decompensation cohort. The most common CAM was unlabeled polyherbal Ayurvedic formulations. Of possible patients with ACLF, 63% self-medicated with CAM based on social media sharing. Mean age ± SD was 51.9 ± 9.9 years, 83% were male patients, median follow-up duration was 173 (range, 14-584) days, median Child-Turcotte-Pugh score was 13 (range, 10-14), Model for End-Stage Liver Disease-sodium score was 30.1 ± 4.8, median chronic liver failure-organ failure (CLIF-C-OF) score was 11 (range, 8-14), and median CLIF-C-ACLF score was 98 (range, 87-127). Portal-based neutrophilic predominant mixed inflammation, hepatocyte ballooning, autoimmune-like features, and severe cholestasis were seen on liver biopsy. Overall, 53% of patients died (median survival 194 days). Baseline overt hepatic encephalopathy and CLIF-C-OF score, total bilirubin, hyponatremia and leukocytosis, and grade of ACLF predicted 1-, 3-, 6- and 12-month mortality, respectively. Conclusion: Possible CAM-DILI-related ACLF has a high mortality. Strict monitoring and identification of CAM use among people with cirrhosis and an integrative public health educational practice can help ameliorate this modifiable risk factor that potentiates heavy liver disease burden and resource use.
Figures
References
-
- Rao KD, Sundararaman T, Bhatnagar A, Gupta G, Kokho P, Jain K. Which doctor for primary health care? Quality of care and non‐physician clinicians in India. Soc Sci Med 2013;84:30‐34. - PubMed
-
- Ministry of AYUSH . Summary of infrastructure facilities under AYUSH; 2010. http://www.ayush.gov.in/infrastructure/summary-infrastructure-facilities.... Published February 15, 2016. Accessed November 18, 2018.
-
- Rastogi S. Ayurveda for comprehensive healthcare. Indian J Med Ethics 2009;6:101‐102. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
