

Simplifying switch to second-line antiretroviral therapy in sub Saharan Africa: predicted effect of using a single viral load to define efavirenz-based first-line failure
- PMID: 31305331
- PMCID: PMC6641111
- DOI: 10.1097/QAD.0000000000002234
Simplifying switch to second-line antiretroviral therapy in sub Saharan Africa: predicted effect of using a single viral load to define efavirenz-based first-line failure
Abstract
Background: Many individuals failing first-line antiretroviral therapy (ART) in sub-Saharan Africa never initiate second-line ART or do so after significant delay. For people on ART with a viral load more than 1000 copies/ml, the WHO recommends a second viral load measurement 3 months after the first viral load and enhanced adherence support. Switch to a second-line regimen is contingent upon a persistently elevated viral load more than 1000 copies/ml. Delayed second-line switch places patients at increased risk for opportunistic infections and mortality.
Methods: To assess the potential benefits of a simplified second-line ART switch strategy, we use an individual-based model of HIV transmission, progression and the effect of ART which incorporates consideration of adherence and drug resistance, to compare predicted outcomes of two policies, defining first-line regimen failure for patients on efavirenz-based ART as either two consecutive viral load values more than 1000 copies/ml, with the second after an enhanced adherence intervention (implemented as per current WHO guidelines) or a single viral load value more than 1000 copies/ml. We simulated a range of setting-scenarios reflecting the breadth of the sub-Saharan African HIV epidemic, taking into account potential delays in defining failure and switch to second-line ART.
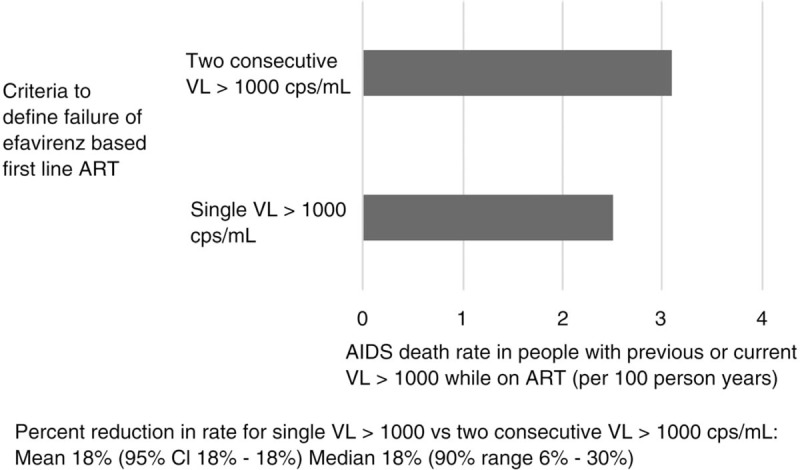
Findings: The use of a single viral load more than 1000 copies/ml to define ART failure would lead to a higher proportion of persons with nonnucleoside reverse-transcriptase inhibitor resistance switched to second-line ART [65 vs. 48%; difference 17% (90% range 14-20%)], resulting in a median 18% reduction in the rate of AIDS-related death over setting scenarios (90% range 6-30%; from a median of 3.1 to 2.5 per 100 person-years) over 3 years. The simplified strategy also is predicted to reduce the rate of AIDS conditions by a median of 31% (90% range 8-49%) among people on first-line ART with a viral load more than 1000 copies/ml in the past 6 months. For a country of 10 million adults (and a median of 880 000 people with HIV), we estimate that this approach would lead to a median of 1322 (90% range 67-3513) AIDS deaths averted per year over 3 years. For South Africa this would represent around 10 215 deaths averted annually.
Interpretation: As a step towards reducing unnecessary mortality associated with delayed second-line ART switch, defining failure of first-line efavirenz-based regimens as a single viral load more than 1000 copies/ml should be considered.
Figures
Comment in
-
HIV viral load algorithm: what are the needs in the field?AIDS. 2020 Jan 1;34(1):159-160. doi: 10.1097/QAD.0000000000002382. AIDS. 2020. PMID: 31693500 Free PMC article. No abstract available.
-
HIV viral load algorithm: what are the needs in the field?: authors' response.AIDS. 2020 Jan 1;34(1):160-162. doi: 10.1097/QAD.0000000000002383. AIDS. 2020. PMID: 31789891 No abstract available.
References
-
- UNAIDS. Fact sheet July 2018 – latest global and regional statistics on the status of the AIDS epidemic. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS; 2018.
-
- World Health Organization. Department of HIV/AIDS – antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach. Geneva, Switzerland: World Health Organization; 2010. - PubMed
-
- Steegen K, Bronze M, Papathanasopoulos MA, van Zyl G, Goedhals D, Variava E, et al. HIV-1 antiretroviral drug resistance patterns in patients failing NNRTI-based treatment: results from a national survey in South Africa. J Antimicrob Chemother 2017; 72:210–219. - PubMed
-
- Gupta RK, Hill A, Sawyer AW, Cozzi-Lepri A, von Wyl V, Yerly S, et al. Virological monitoring and resistance to first-line highly active antiretroviral therapy in adults infected with HIV-1 treated under WHO guidelines: a systematic review and meta-analysis. Lancet Infect Dis 2009; 9:409–417. - PubMed
-
- World Health Organization; United States Centers for Disease Control and Prevention & The Global Fund to Fight AIDS Tuberculosis and Malaria. HIV drug resistance report 2017. Geneva, Switzerland: World Health Organization; 2017.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
