

The clinical application value of multi-slice spiral CT enhanced scans combined with multiplanar reformations images in preoperative T staging of rectal cancer
- PMID: 31305437
- PMCID: PMC6641797
- DOI: 10.1097/MD.0000000000016374
The clinical application value of multi-slice spiral CT enhanced scans combined with multiplanar reformations images in preoperative T staging of rectal cancer
Abstract
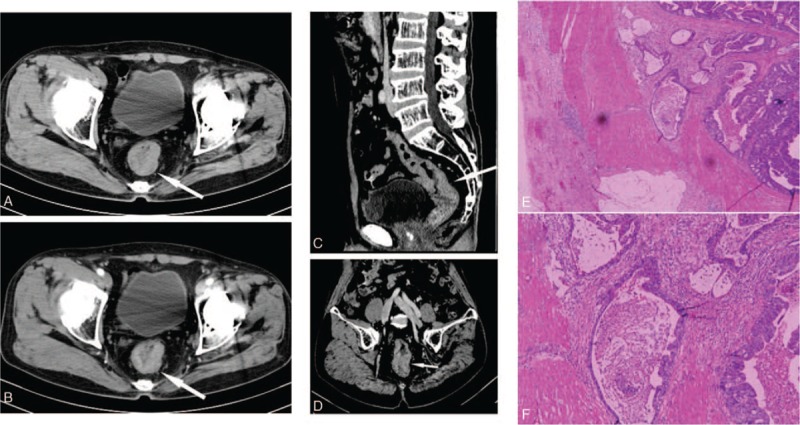
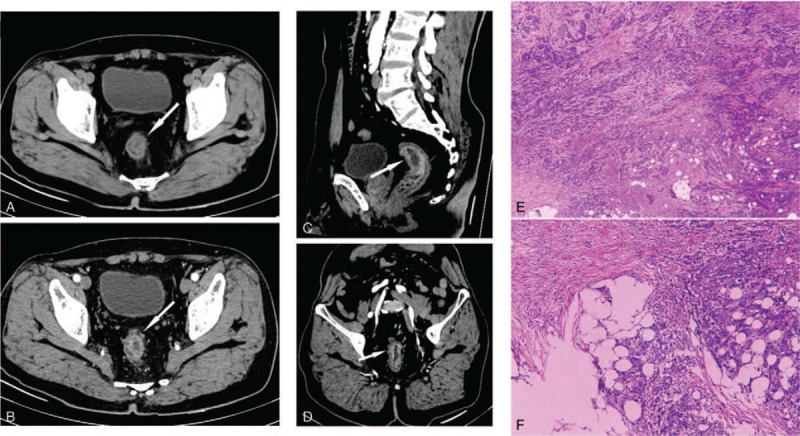
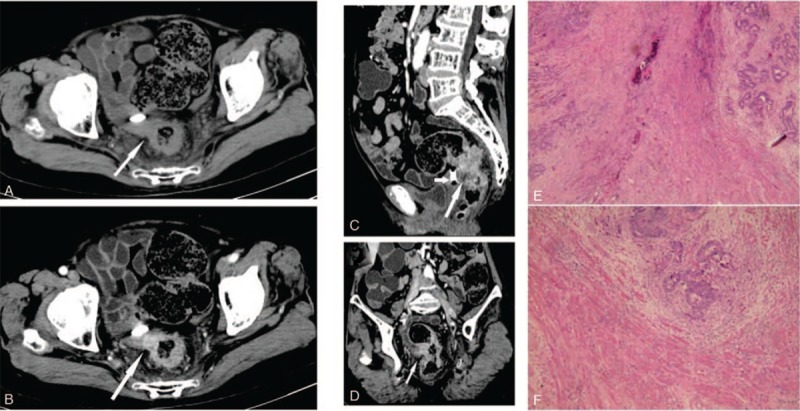
This study aims to evaluate the diagnostic accuracy and clinical application value of multi-slice spiral CT (MSCT) enhanced scans combined with multiplanar reformations (MPRs) images compared with postoperative pathological results in preoperative T staging of rectal cancer.One hundred sixty-eight consecutive patients with rectal cancer were admitted in our hospital between January 2013 and October 2018. Conventional MSCT plain scans, multi-phase dynamic contrast-enhanced scans, and MPRs were performed in all patients before surgical operation. The preoperative T staging of the rectal cancer lesions was evaluated using MSCT enhanced scans combined with MPRs, which was verified by postoperative pathological results. The diagnostic accuracy of MSCT enhanced scans combined with MPRs in evaluating T staging of the rectal cancer lesions were analyzed by χ test and Kappa test.Compared with postoperative pathology, T staging using MSCT enhanced scans combined with MPRs had overall accuracy of 85.7%. Consistency between MSCT enhanced scans combined with MPRs and postoperative pathological staging was effective for T staging (Kappa = 0.658, χ = 4.200, P = .122).Conventional MSCT enhanced scans combined with MPRs are simple and feasible. It is consistent with the pathological diagnosis of evaluating T staging in the rectal cancer lesions. It can provide reliable imaging evidence for the preoperative evaluation of primary rectal cancer, especially in patients with magnetic resonance imaging (MRI) contraindications, or in grass-roots hospitals due to lack of MRI equipment.
Conflict of interest statement
The authors have no conflicts of interests to disclose.
Figures
References
-
- Gu J, Wang JP, Zhang SZ, et al. Chinese Expert Group Criteria for Diagnosis and Treatment of Colorectal Cancer (2017 Edition) of National Health and Family Planning Commission of the People's Republic of China. Chinese Criteria for Diagnosis and Treatment of Colorectal Cancer (2017 Edition). Chin J Clin (Electronic Edition) 2018;12:3–19. [Chinese].
-
- Du LB, Li HZ, Wang YQ, et al. Report of colorectal cancer incidence and mortality in China, 2013. Zhonghua Zhong Liu Za Zhi 2017;39:701–6. [Chinese]. - PubMed
-
- Siegel RL, Miller KD, Fedewa SA, et al. Colorectal cancer statistics. CA Cancer J Clin 2017;67:177–93. 2017. - PubMed
-
- Wang L, Liu ZH, Wang JP. Current status of diagnosis and treatment of colorectal cancer in China. Chin J Exp Surg 2015;32:677–9. [Chinese].
MeSH terms
LinkOut - more resources
Full Text Sources
