

An interactive nomogram to predict healthcare-associated infections in ICU patients: A multicenter study in GuiZhou Province, China
- PMID: 31306445
- PMCID: PMC6629073
- DOI: 10.1371/journal.pone.0219456
An interactive nomogram to predict healthcare-associated infections in ICU patients: A multicenter study in GuiZhou Province, China
Abstract
Objective: To develop and validate an interactive nomogram to predict healthcare-associated infections (HCAIs) in the intensive care unit (ICU).
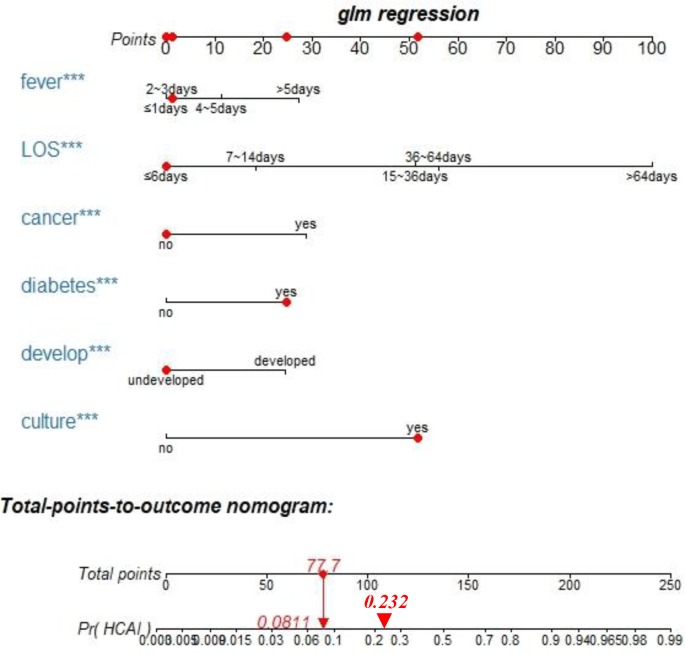
Methods: A multicenter retrospective study was conducted to review 2017 data from six hospitals in Guizhou Province, China. A total of 1,782 ICU inpatients were divided into either a training set (n = 1,189) or a validation set (n = 593). The patients' demographic characteristics, basic clinical features from the previous admission, and their need for bacterial culture during the current admission were extracted from electronic medical records of the hospitals to predict HCAI. Univariate and multivariable analyses were used to identify independent risk factors of HCAI in the training set. The multivariable model's performance was evaluated in both the training set and the validation set, and an interactive nomogram was constructed according to multivariable regression model. Moreover, the interactive nomogram was used to predict the possibility of a patient developing an HCAI based on their prior admission data. Finally, the clinical usefulness of the interactive nomogram was estimated by decision analysis using the entire dataset.
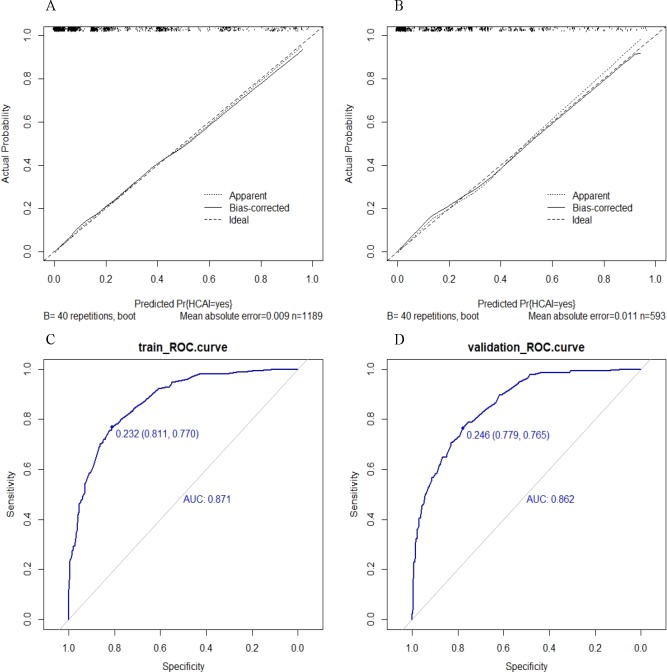
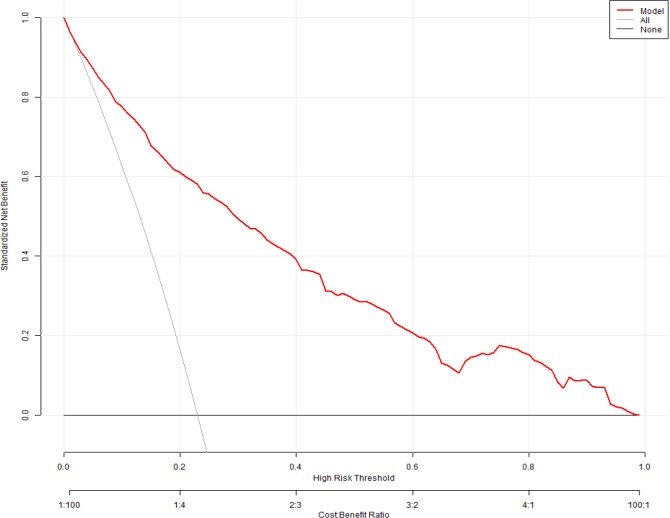
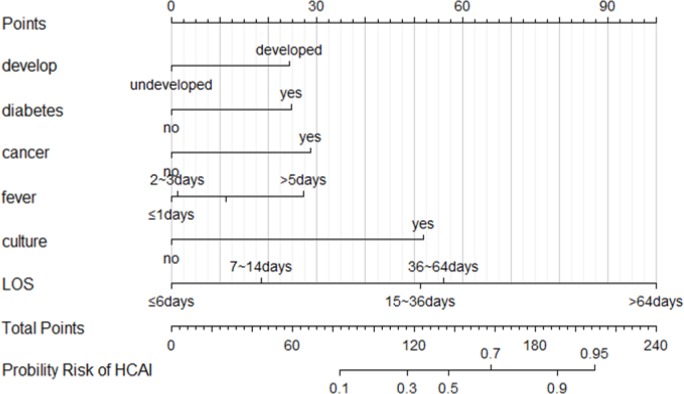
Results: The nomogram model included factor development (local economic development levels), length of stay (LOS; days of hospital stay), fever (days of persistent fever), diabetes (history of diabetes), cancer (history of cancer) and culture (the need for bacterial culture). The model showed good calibration and discrimination in the training set [area under the curve (AUC), 0.871; 95% confidence interval (CI), 0.848-0.894] and in the validation set (AUC, 0.862; 95% CI, 0.829-0.895). The decision curve demonstrated the clinical usefulness of our interactive nomogram.
Conclusions: The developed interactive nomogram is a simple and practical instrument for quantifying the individual risk of HCAI and promptly identifying high-risk patients.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Risk factors and predictive model for nosocomial infections by extensively drug-resistant Acinetobacter baumannii.Front Cell Infect Microbiol. 2024 Sep 30;14:1475428. doi: 10.3389/fcimb.2024.1475428. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 39403207 Free PMC article.
-
Development and validation of a predictive model for pulmonary infection risk in patients with traumatic brain injury in the ICU: a retrospective cohort study based on MIMIC-IV.BMJ Open Respir Res. 2024 Jul 31;11(1):e002263. doi: 10.1136/bmjresp-2023-002263. BMJ Open Respir Res. 2024. PMID: 39089740 Free PMC article.
-
Development and application of a risk nomogram for the prediction of risk of carbapenem-resistant Acinetobacter baumannii infections in neuro-intensive care unit: a mixed method study.Antimicrob Resist Infect Control. 2024 Jun 13;13(1):62. doi: 10.1186/s13756-024-01420-6. Antimicrob Resist Infect Control. 2024. PMID: 38867312 Free PMC article.
-
[Evaluation of Infections in Intensive Care Units: A Multicentre Point-Prevalence Study].Mikrobiyol Bul. 2019 Oct;53(4):364-373. doi: 10.5578/mb.68665. Mikrobiyol Bul. 2019. PMID: 31709934 Review. Turkish.
-
Development and validation of a nomogram for predicting the risk of nursing home-acquired pneumonia.Eur Rev Med Pharmacol Sci. 2022 Nov;26(22):8276-8288. doi: 10.26355/eurrev_202211_30360. Eur Rev Med Pharmacol Sci. 2022. PMID: 36459011 Review.
Cited by
-
Prediction of nosocomial infection incidence in the Department of Critical Care Medicine of Guizhou Province with a time series model.Ann Transl Med. 2020 Jun;8(12):758. doi: 10.21037/atm-20-4171. Ann Transl Med. 2020. PMID: 32647683 Free PMC article.
References
-
- Allegranzi B, Nejad SB, Combescure C, Graafmans W, Attar H, Donaldson L, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011;377(9761):228–41. 10.1016/S0140-6736(10)61458-4 PubMed PMID: WOS:000286696400030. - DOI - PubMed
-
- Zarb P, Coignard B, Griskeviciene J, Muller A, Vankerckhoven V, Weist K, et al. The European Centre for Disease Prevention and Control (ECDC) pilot point prevalence survey of healthcare-associated infections and antimicrobial use. Eurosurveillance. 2012;17(46):4–19. PubMed PMID: WOS:000311885000002. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
