

Cost-effectiveness of scaling-up HCV prevention and treatment in the United States for people who inject drugs
- PMID: 31307116
- PMCID: PMC7751348
- DOI: 10.1111/add.14731
Cost-effectiveness of scaling-up HCV prevention and treatment in the United States for people who inject drugs
Abstract
Aims: To examine the cost-effectiveness of hepatitis C virus (HCV) treatment of people who inject drugs (PWID), combined with medication-assisted treatment (MAT) and syringe-service programs (SSP), to tackle the increasing HCV epidemic in the United States.
Design: HCV transmission and disease progression models with cost-effectiveness analysis using a health-care perspective.
Setting: Rural Perry County, KY (PC) and urban San Francisco, CA (SF), USA. Compared with PC, SF has a greater proportion of PWID with access to MAT or SSP. HCV treatment of PWID is negligible in both settings.
Participants: PWID data were collected between 1998 and 2015 from Social Networks Among Appalachian People, U Find Out, Urban Health Study and National HIV Behavioral Surveillance System studies.
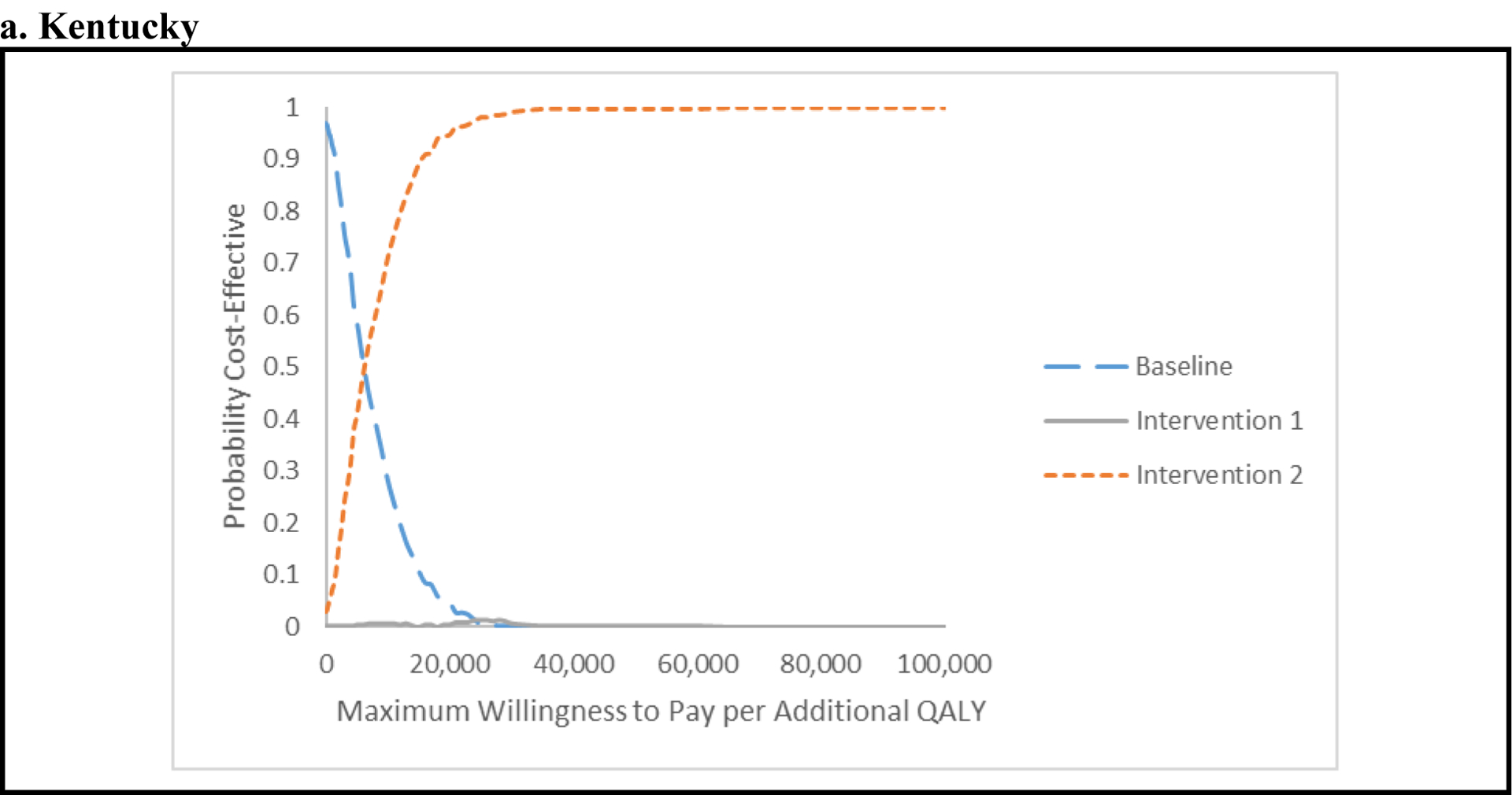
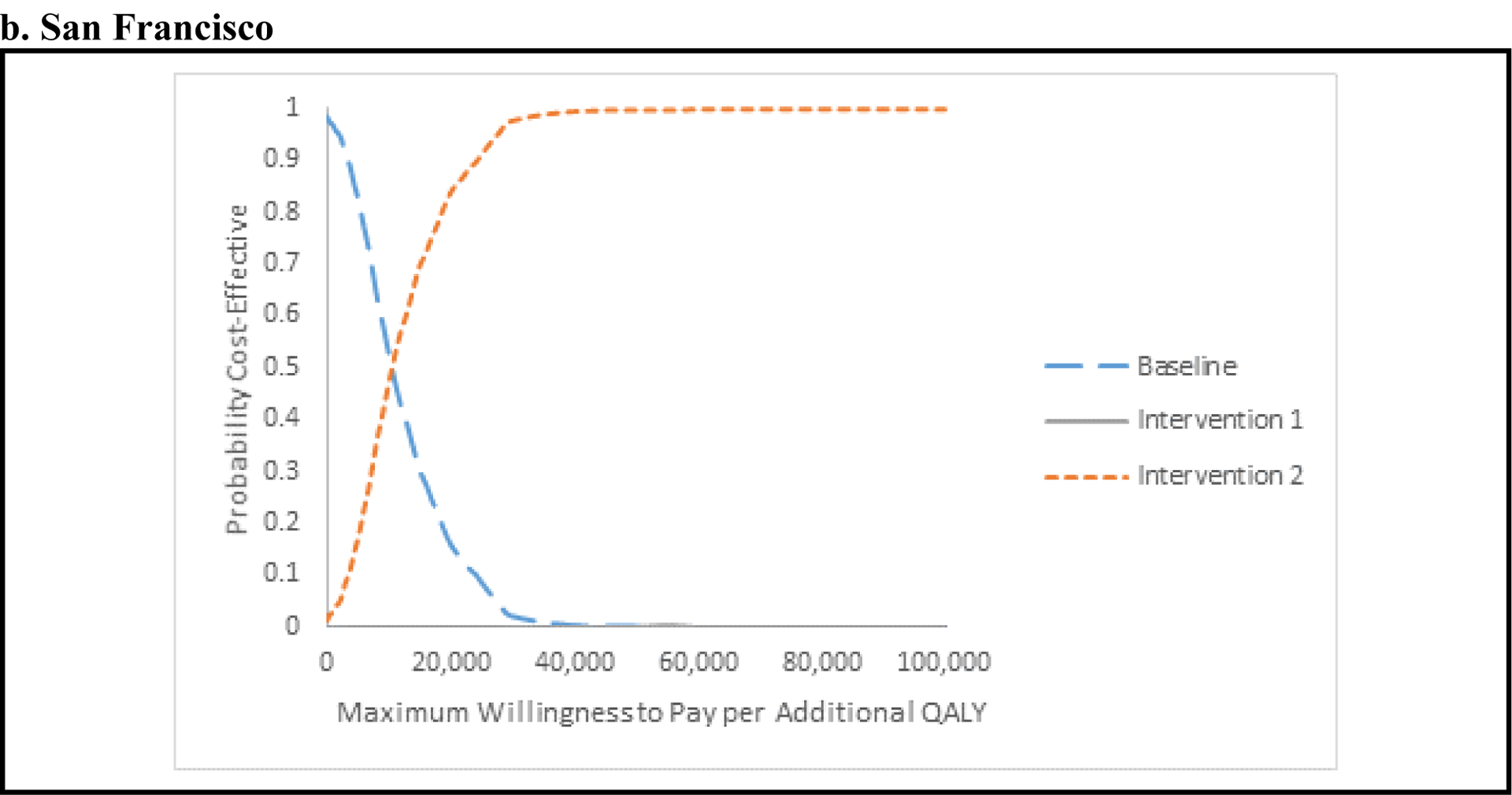
Interventions and comparator: Three intervention scenarios modeled: baseline-existing SSP and MAT coverage with HCV screening and treatment with direct-acting antiviral for ex-injectors only as per standard of care; intervention 1-scale-up of SSP and MAT without changes to treatment; and intervention 2-scale-up as intervention 1 combined with HCV screening and treatment for current PWID.
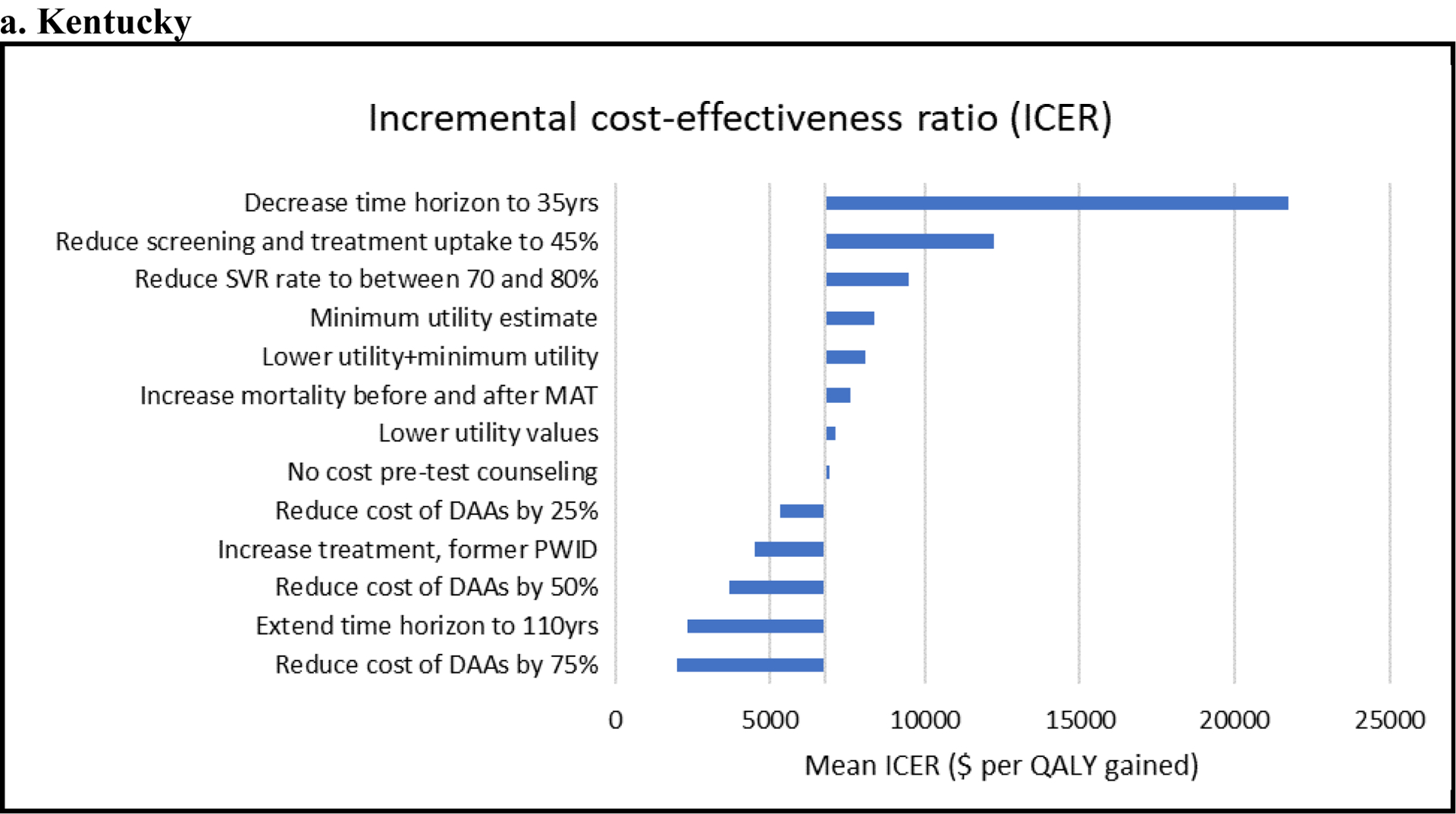
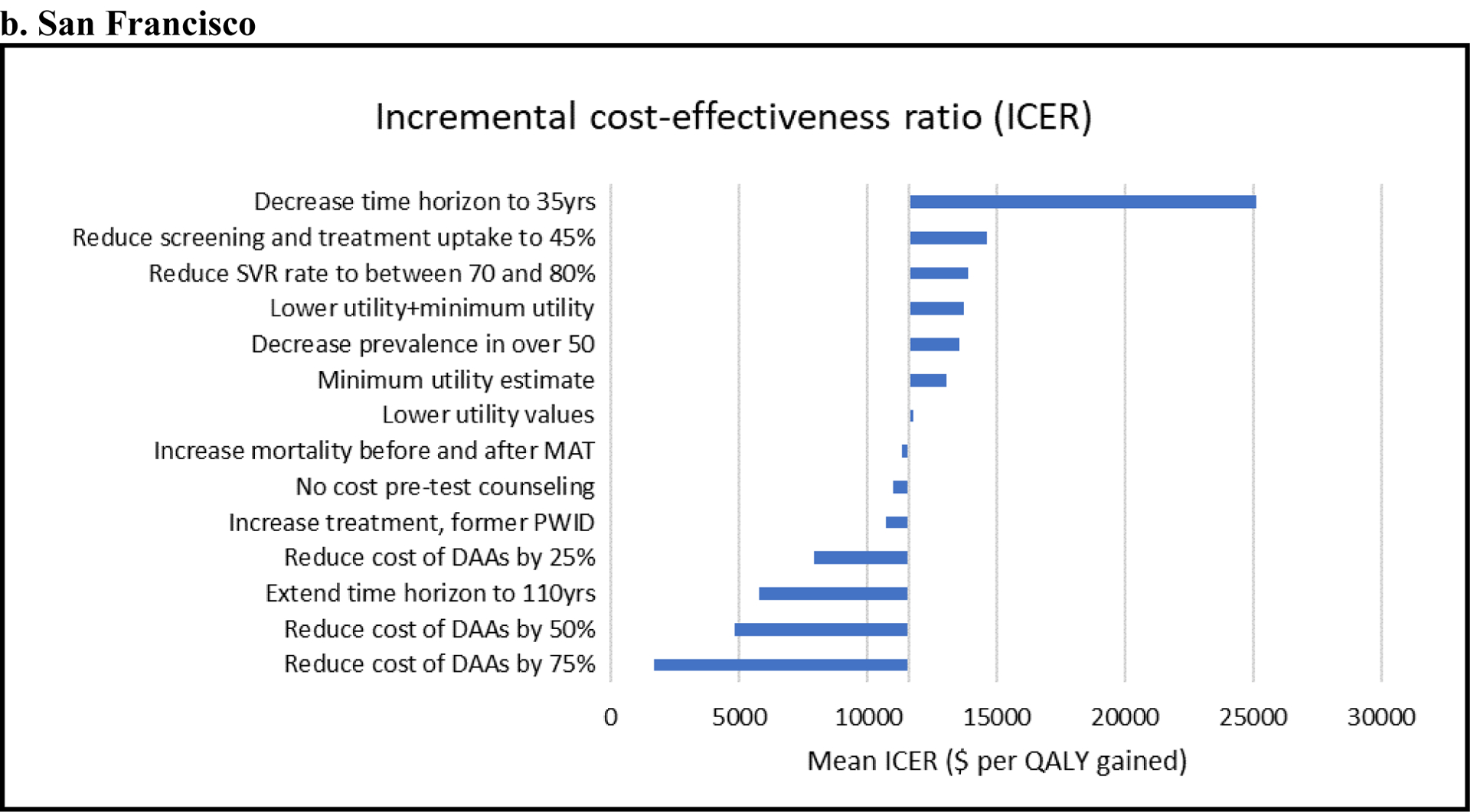
Measurements: Incremental cost-effectiveness ratios (ICERs) and uncertainty using cost-effectiveness acceptability curves. Benefits were measured in quality-adjusted life-years (QALYs).
Findings: For both settings, intervention 2 is preferred to intervention 1 and the appropriate comparator for intervention 2 is the baseline scenario. Relative to baseline, for PC intervention 2 averts 1852 more HCV infections, increases QALYS by 3095, costs $21.6 million more and has an ICER of $6975/QALY. For SF, intervention 2 averts 36 473 more HCV infections, increases QALYs by 7893, costs $872 million more and has an ICER of $11 044/QALY. The cost-effectiveness of intervention 2 was robust to several sensitivity analysis.
Conclusions: Hepatitis C screening and treatment for people who inject drugs, combined with medication-assisted treatment and syringe-service programs, is a cost-effective strategy for reducing hepatitis C burden in the United States.
Keywords: Cost-effectiveness analysis; direct-acting antiviral HCV treatment; hepatitis C; medication-assisted treatment; opioid modeling; people who inject drugs; syringe-service programs.
© 2019 Society for the Study of Addiction.
Figures
Comment in
-
Commentary on Barbosa et al. (2019): The value of using community simulation modeling to achieve HCV elimination targets in people who inject drugs.Addiction. 2019 Dec;114(12):2279-2280. doi: 10.1111/add.14807. Epub 2019 Oct 23. Addiction. 2019. PMID: 31646686 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention. Viral Hepatitis Surveillance United States, 2015. Available from: https://www.cdc.gov/hepatitis/statistics/2015surveillance/pdfs/2015HepSu..., Archived at: http://www.webcitation.org/78PtzMtMG on May 16th, 2019.
-
- Centers for Disease Control and Prevention. Surveillance for Viral Hepatitis – United States, 2013. Available from: http://www.cdc.gov/hepatitis/statistics/2013surveillance/index.htm, Archived at http://www.webcitation.org/78Q7FBGbt on May 16th, 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
