

MRI evaluation of cerebrovascular reactivity in obstructive sleep apnea
- PMID: 31307289
- PMCID: PMC7238371
- DOI: 10.1177/0271678X19862182
MRI evaluation of cerebrovascular reactivity in obstructive sleep apnea
Abstract
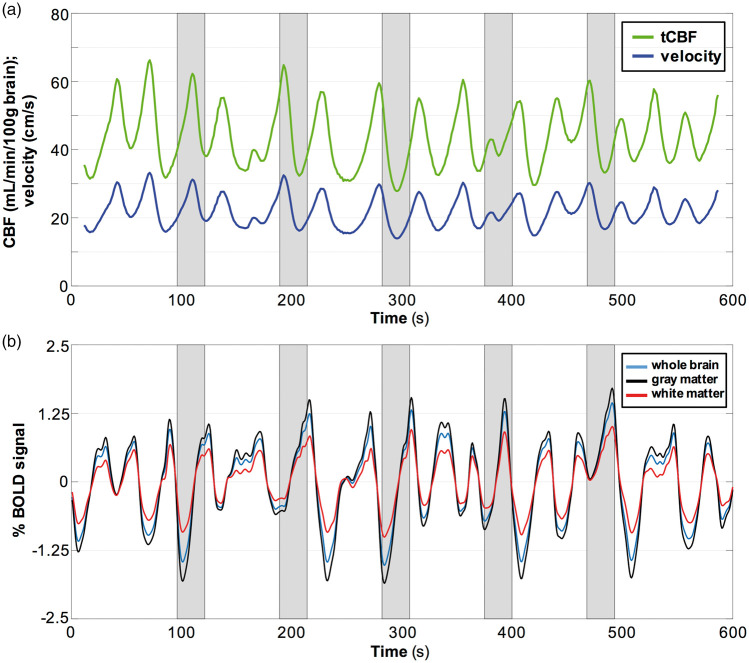
Obstructive sleep apnea (OSA) is characterized by intermittent obstruction of the airways during sleep. Cerebrovascular reactivity (CVR) is an index of cerebral vessels' ability to respond to a vasoactive stimulus, such as increased CO2. We hypothesized that OSA alters CVR, expressed as a breath-hold index (BHI) defined as the rate of change in CBF or BOLD signal during a controlled breath-hold stimulus mimicking spontaneous apneas by being both hypercapnic and hypoxic. In 37 OSA and 23 matched non sleep apnea (NSA) subjects, we obtained high temporal resolution CBF and BOLD MRI data before, during, and between five consecutive BH stimuli of 24 s, each averaged to yield a single BHI value. Greater BHI was observed in OSA relative to NSA as derived from whole-brain CBF (78.6 ± 29.6 vs. 60.0 ± 20.0 mL/min2/100 g, P = 0.010) as well as from flow velocity in the superior sagittal sinus (0.48 ± 0.18 vs. 0.36 ± 0.10 cm/s2, P = 0.014). Similarly, BOLD-based BHI was greater in OSA in whole brain (0.19 ± 0.08 vs. 0.15 ± 0.03%/s, P = 0.009), gray matter (0.22 ± 0.09 vs. 0.17 ± 0.03%/s, P = 0.011), and white matter (0.14 ± 0.06 vs. 0.10 ± 0.02%/s, P = 0.010). The greater CVR is not currently understood but may represent a compensatory mechanism of the brain to maintain oxygen supply during intermittent apneas.
Keywords: BOLD; breath-hold index; cerebrovascular reactivity; obstructive sleep apnea; radial phase-contrast MRI.
Figures



Similar articles
-
MRI evaluation of cerebral metabolic rate of oxygen (CMRO2) in obstructive sleep apnea.J Cereb Blood Flow Metab. 2022 Jun;42(6):1049-1060. doi: 10.1177/0271678X211071018. Epub 2022 Jan 7. J Cereb Blood Flow Metab. 2022. PMID: 34994242 Free PMC article.
-
Impaired cerebrovascular reactivity in obstructive sleep apnea: a case-control study.Sleep Med. 2018 Mar;43:7-13. doi: 10.1016/j.sleep.2017.10.010. Epub 2017 Nov 15. Sleep Med. 2018. PMID: 29482816
-
Evaluation of Cerebrovascular Reactivity in Subjects with and without Obstructive Sleep Apnea.J Stroke Cerebrovasc Dis. 2018 Jan;27(1):162-168. doi: 10.1016/j.jstrokecerebrovasdis.2017.08.015. Epub 2017 Sep 13. J Stroke Cerebrovasc Dis. 2018. PMID: 28918088
-
Cerebrovascular reactivity in young subjects with sleep apnea.Sleep. 2015 Feb 1;38(2):241-50. doi: 10.5665/sleep.4406. Sleep. 2015. PMID: 25409111 Free PMC article.
-
Human cerebral blood flow control during hypoxia: focus on chronic pulmonary obstructive disease and obstructive sleep apnea.J Appl Physiol (1985). 2017 Nov 1;123(5):1350-1361. doi: 10.1152/japplphysiol.00352.2017. Epub 2017 Aug 10. J Appl Physiol (1985). 2017. PMID: 28798199 Review.
Cited by
-
Altered regional cerebral blood flow in obstructive sleep apnea is associated with sleep fragmentation and oxygen desaturation.J Cereb Blood Flow Metab. 2021 Oct;41(10):2712-2724. doi: 10.1177/0271678X211012109. Epub 2021 Apr 28. J Cereb Blood Flow Metab. 2021. PMID: 33906511 Free PMC article.
-
MRI evaluation of cerebral metabolic rate of oxygen (CMRO2) in obstructive sleep apnea.J Cereb Blood Flow Metab. 2022 Jun;42(6):1049-1060. doi: 10.1177/0271678X211071018. Epub 2022 Jan 7. J Cereb Blood Flow Metab. 2022. PMID: 34994242 Free PMC article.
-
Acute e-cig inhalation impacts vascular health: a study in smoking naïve subjects.Am J Physiol Heart Circ Physiol. 2021 Jan 1;320(1):H144-H158. doi: 10.1152/ajpheart.00628.2020. Epub 2020 Nov 20. Am J Physiol Heart Circ Physiol. 2021. PMID: 33216614 Free PMC article.
-
Concurrent evaluation of cerebral oxygen metabolism and upper airway architecture via temporally resolved MRI.J Cereb Blood Flow Metab. 2025 May 25:271678X251345293. doi: 10.1177/0271678X251345293. Online ahead of print. J Cereb Blood Flow Metab. 2025. PMID: 40415373 Free PMC article.
-
Body mass index and neuropsychological and emotional variables: joint contribution for the screening of sleep apnoea syndrome in obese.Sleep Sci. 2021 Jan-Mar;14(1):19-26. doi: 10.5935/1984-0063.20200030. Sleep Sci. 2021. PMID: 34104333 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
