

Clinical and microbiologic investigation of an expedited peri-implantitis dog model: an animal study
- PMID: 31307461
- PMCID: PMC6632201
- DOI: 10.1186/s12903-019-0837-y
Clinical and microbiologic investigation of an expedited peri-implantitis dog model: an animal study
Abstract
Background: Animal studies are pivotal in allowing experimentation to identify efficacious treatment protocols for resolution of peri-implantitis. The purpose of this investigation was to characterize an expedited dog peri-implantitis model clinically, radiographically, and microbiologically.
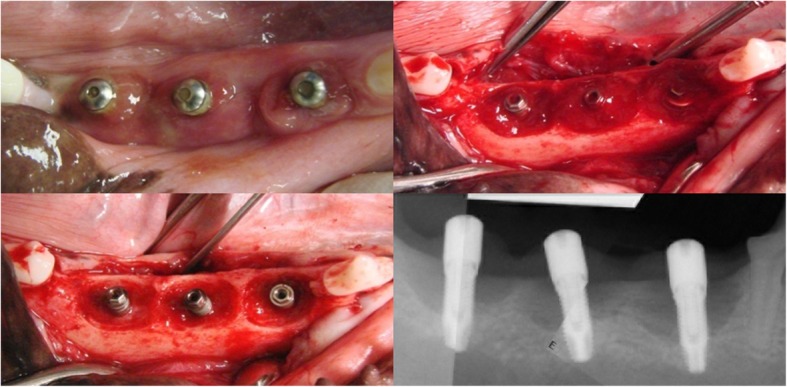
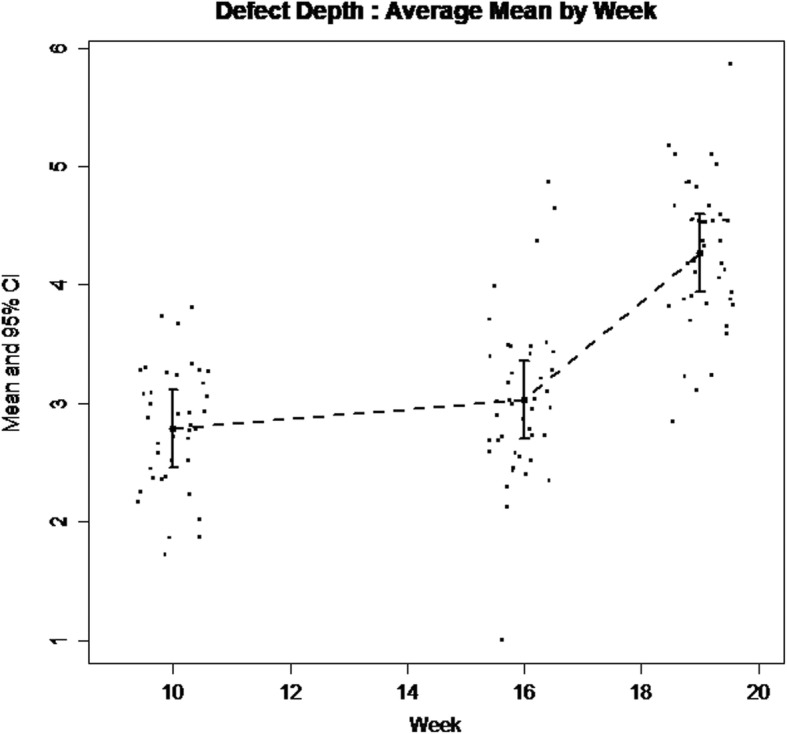
Methods: Eight hound dogs underwent extractions (week 0) and implant (3.3 × 8.5 mm) placement with simultaneous surgical defect creation and ligature placement for induction of peri-implantitis (week 10). Ligatures were replaced at 6 weeks (week 16) and removed after 9 weeks (week 19) when supporting bone loss involved approximately 50% of the peri-implant bone. Microbial samples from the defects and healthy control implant sites collected at week 19 were analyzed utilizing a microarray. Clinical measures of inflammation were obtained and radiographic bone loss was measured from periapical radiographs. Radiographic depth and width measurements of bony defect were repeated at weeks 10 (baseline), 16, and 19. Canonical analysis of principal coordinates was used to visualize overall differences in microbial abundance between peri-implantitis and healthy implants.
Results: This accelerated disease protocol led to intrabony defect creation with a mean depth and width of 4.3 mm and 3.5 mm, respectively after 9 weeks of ligature placement. Microbial identification revealed 59 total bacteria in peri-implant sites, 21 of which were only present in peri-implant sites as compared to healthy controls. Overall microbial beta diversity (microbial between-sample compositional diversity) differed between peri-implantitis and healthy implants (p = 0.009).
Conclusions: Within the limitations of this study, this protocol led to expedited generation of peri-implant defects with a microbial profile indicative of a shift to disease and defect patterns conducive to regenerative treatment. However, the possibility of potential spontaneous resolution of lesions due to the lack of a chronicity interval as compared to chronic disease models need to be further clarified and considered during preclinical peri-implantitis model selection.
Keywords: Dental implant; Expedited dog model; Peri-implantitis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures






References
-
- Konstantinidis I, Kotsakis GA, Gerdes S, Walter M. A cross-sectional study on the prevalence and risk indicators of peri-implant diseases. Eur J Oral Implantol. 2015;8(1):75–88. - PubMed
-
- Esposito M, Grusovin MG, Kakisis I, Coulthard P, Worthington HV. Interventions for replacing missing teeth: treatment of perimplantitis. Cochrane Database Syst Rev. 2008;2:CD004970. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
