

Diagnostic performance of cardiovascular magnetic resonance native T1 and T2 mapping in pediatric patients with acute myocarditis
- PMID: 31307467
- PMCID: PMC6631973
- DOI: 10.1186/s12968-019-0550-7
Diagnostic performance of cardiovascular magnetic resonance native T1 and T2 mapping in pediatric patients with acute myocarditis
Abstract
Background: Multiple studies in adult patients suggest that tissue mapping performed by cardiovascular magnetic resonance (CMR) has excellent diagnostic accuracy in acute myocarditis, however, these techniques have not been studied in depth in children.
Methods: CMR data on 23 consecutive pediatric patients from 2014 to 2017 with a clinical diagnosis of acute myocarditis were retrospectively analyzed and compared to 39 healthy controls. The CMR protocol included native T1, T2, and extracellular volume fraction (ECV) in addition to standard Lake Louise Criteria (LLC) parameters on a 1.5 T scanner.
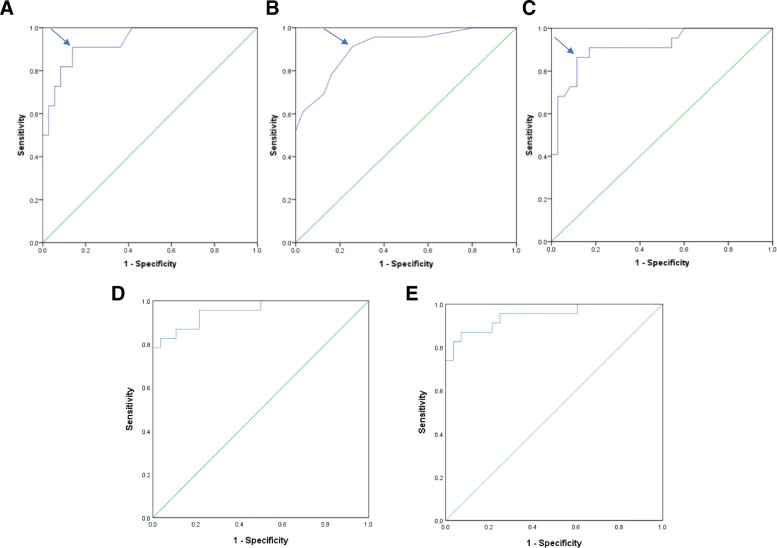
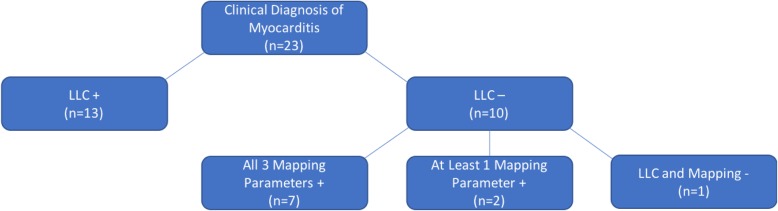
Results: Mean global values for novel mapping parameters were significantly elevated in patients with clinically suspected acute myocarditis compared to controls, with native T1 1098 ± 77 vs 990 ± 34 ms, T2 52.8 ± 4.6 ms vs 46.7 ± 2.6 ms, and ECV 29.8 ± 5.1% vs 23.3 ± 2.6% (all p-values < 0.001). Ideal cutoff values were generated using corresponding ROC curves and were for global T1 1015 ms (AUC 0.936, sensitivity 91%, specificity 86%), for global T2 48.5 ms (AUC 0.908, sensitivity 91%, specificity 74%); and for ECV 25.9% (AUC 0.918, sensitivity 86%, specificity 89%). While the diagnostic yield of the LLC was 57% (13/23) in our patient cohort, 70% (7/10) of patients missed by the LLC demonstrated abnormalities across all three global mapping parameters (native T1, T2, and ECV) and another 20% (2/10) of patients demonstrated at least one abnormal mapping value.
Conclusions: Similar to findings in adults, pediatric patients with acute myocarditis demonstrate abnormal CMR tissue mapping values compared to controls. Furthermore, we found CMR parametric mapping techniques measurably increased CMR diagnostic yield when compared with conventional LLC alone, providing additional sensitivity and specificity compared to historical references. Routine integration of these techniques into imaging protocols may aid diagnosis in children.
Keywords: Cardiovascular magnetic resonance; Extracellular volume; Myocarditis; Pediatrics; T1 mapping; T2 mapping.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Foerster SR, Canter CE, Cinar A, Sleeper LA, Webber SA, Pahl E, et al. Ventricular remodeling and survival are more favorable for myocarditis than for idiopathic dilated cardiomyopathy in childhood: an outcomes study from the pediatric cardiomyopathy registry. Circ Heart Fail. 2010;3(6):689–697. doi: 10.1161/CIRCHEARTFAILURE.109.902833. - DOI - PubMed
-
- Bohnen S, Radunski UK, Lund GK, Kandolf R, Stehning C, Schnackenburg B, et al. Performance of t1 and t2 mapping cardiovascular magnetic resonance to detect active myocarditis in patients with recent-onset heart failure. Circulation Cardiovascular imaging. 2015;8(6). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
