

Preoperative breast MRI features associated with positive or close margins in breast-conserving surgery
- PMID: 31307644
- PMCID: PMC6662937
- DOI: 10.1016/j.ejrad.2019.06.011
Preoperative breast MRI features associated with positive or close margins in breast-conserving surgery
Abstract
Purpose: To determine preoperative magnetic resonance imaging (MRI) features associated with positive or close margins in patients with breast cancer who underwent breast-conserving surgery (BCS).
Materials and methods: A retrospective review identified 249 patients with invasive ductal carcinoma (IDC) who underwent preoperative MRI and BCS as a primary procedure between 2008 and 2010. The MR images were reviewed for descriptions of findings with no new interpretations made. Margins were defined as positive (tumor touching the inked specimen margin), close (<2 mm tumor-free margin), or negative (≥2 mm tumor-free margin). Multivariate logistic regression analysis was performed to evaluate imaging and clinical factors predictive of positive or close margins.
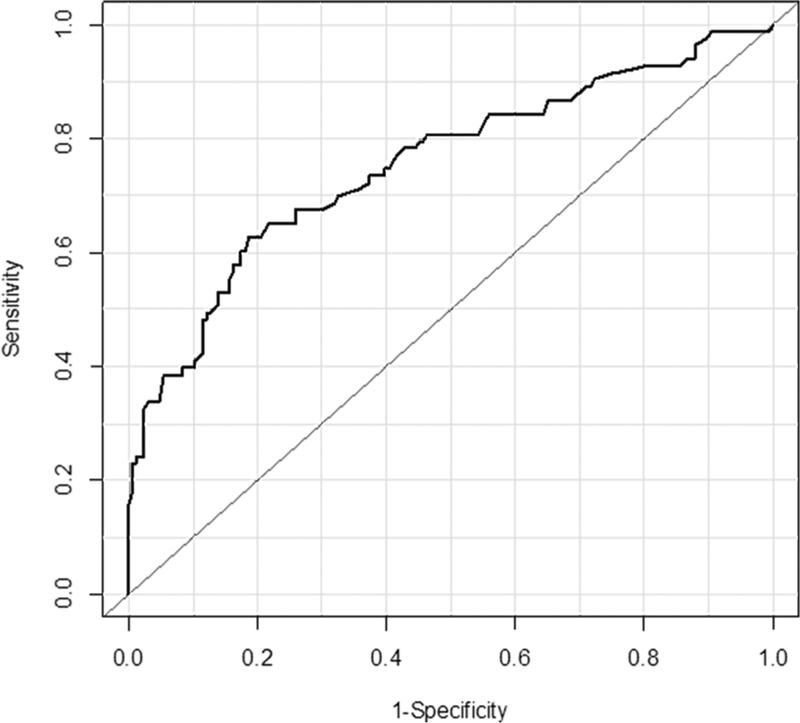
Results: Of the 249 patients, 83 (33.3%) had positive or close margins and 166 (66.7%) had negative margins on the initial BCS specimen. Multivariate analysis showed that multifocal disease (odds ratio, 4.8; 95% CI, 1.9-12.2; p = 0.001), nonmass enhancement lesion (odds ratio, 3.0; 95% CI, 1.5-6.2, p = 0.003), greater background parenchymal enhancement (odds ratio, 2.5; 95% CI, 1.1-5.6; p = 0.023), larger lesion size (odds ratio, 1.3; 95% CI, 1.0-1.7, p = 0.032), and presence of ductal carcinoma in situ on needle biopsy (odds ratio, 2.4; 95% CI, 1.3-4.6; p = 0.008) were independent predictors of positive or close margins.
Conclusions: Multifocal disease, nonmass enhancement lesion, or greater background parenchymal enhancement on preoperative breast MRI were significantly associated with positive or close margins. Identifying these MRI features before surgery can be helpful to reduce the reoperation rate in BCS.
Keywords: Breast cancer; Breast-conserving surgery; Preoperative MRI; Resection margins.
Copyright © 2019 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures


Similar articles
-
Preoperative Magnetic Resonance Imaging Features Associated with Positive Resection Margins in Patients with Invasive Lobular Carcinoma.Korean J Radiol. 2020 Aug;21(8):946-954. doi: 10.3348/kjr.2019.0674. Korean J Radiol. 2020. PMID: 32677379 Free PMC article.
-
MRI predictors of tumor-positive margins after breast-conserving surgery.Clin Imaging. 2019 Sep-Oct;57:45-49. doi: 10.1016/j.clinimag.2019.05.006. Epub 2019 May 15. Clin Imaging. 2019. PMID: 31128385
-
External validation and modification of nomogram for predicting positive resection margins before breast conserving surgery.Breast Cancer Res Treat. 2020 Sep;183(2):373-380. doi: 10.1007/s10549-020-05779-z. Epub 2020 Jul 9. Breast Cancer Res Treat. 2020. PMID: 32647937
-
Positive Margin Rates After Breast-Conserving Surgery by Histologic Subtype: A Systematic Review and Meta-analysis Evaluating the Impact of Oncoplastic Surgery.Ann Surg Oncol. 2025 Jul;32(7):4899-4909. doi: 10.1245/s10434-025-17329-2. Epub 2025 Apr 24. Ann Surg Oncol. 2025. PMID: 40272667 Free PMC article.
-
Close/positive margins after breast-conserving therapy: additional resection or no resection?Breast. 2013 Aug;22 Suppl 2:S115-7. doi: 10.1016/j.breast.2013.07.022. Breast. 2013. PMID: 24074771 Review.
Cited by
-
Accuracy of Breast MRI for Surgical Planning After Neoadjuvant Therapy for Patients with Invasive Lobular Carcinoma.Ann Surg Oncol. 2025 Jun 27. doi: 10.1245/s10434-025-17735-6. Online ahead of print. Ann Surg Oncol. 2025. PMID: 40576899
-
Preoperative magnetic resonance imaging identify feasibility of breast-conserving surgery for breast cancer patients.Gland Surg. 2024 May 30;13(5):640-653. doi: 10.21037/gs-23-509. Epub 2024 May 27. Gland Surg. 2024. PMID: 38845837 Free PMC article.
-
The influencing factors and prognosis analysis of positive initial margin in intraoperative frozen section during breast-conserving surgery.Eur J Med Res. 2025 May 14;30(1):384. doi: 10.1186/s40001-025-02631-2. Eur J Med Res. 2025. PMID: 40369612 Free PMC article.
-
[Diagnosis of breast diseases in a certified breast center].Radiologe. 2021 Feb;61(2):137-149. doi: 10.1007/s00117-020-00791-2. Epub 2021 Jan 6. Radiologe. 2021. PMID: 33404685 Review. German.
-
Immediate or delayed oncoplastic surgery after breast conserving surgery at the Netherlands Cancer Institute: a cohort study of 251 cases.Breast Cancer Res Treat. 2023 Apr;198(2):295-307. doi: 10.1007/s10549-022-06841-8. Epub 2023 Jan 24. Breast Cancer Res Treat. 2023. PMID: 36690822
References
-
- Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med 347 (2002) 1227–1232. - PubMed
-
- Landercasper J, Whitacre E, Degnim AC, Al-Hamadani M. Reasons for re-excision after lumpectomy for breast cancer: insight from the American Society of Breast Surgeons Mastery(SM) database. Ann Surg Oncol 21 (2014) 3185–3191. - PubMed
-
- Clarke M, Collins R, Darby S, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomized trials. Lancet 366 (2005) 2087–2106. - PubMed
-
- Wilke LG, Czechura T, Wang C, et al. Repeat surgery after breast conservation for the treatment of stage 0 to II breast carcinoma: a report from the National Cancer Data Base, 2004–2010. JAMA Surg 149 (2014) 1296–1305. - PubMed
