

Long-Term Outcomes after Acute Rejection in Kidney Transplant Recipients: An ANZDATA Analysis
- PMID: 31308074
- PMCID: PMC6727270
- DOI: 10.1681/ASN.2018111101
Long-Term Outcomes after Acute Rejection in Kidney Transplant Recipients: An ANZDATA Analysis
Abstract
Background: Declining rates of acute rejection (AR) and the high rate of 1-year graft survival among patients with AR have prompted re-examination of AR as an outcome in the clinic and in trials. Yet AR and its treatment may directly or indirectly affect longer-term outcomes for kidney transplant recipients.
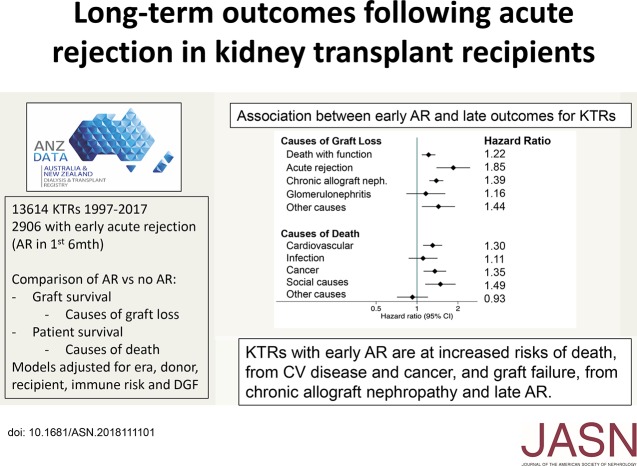
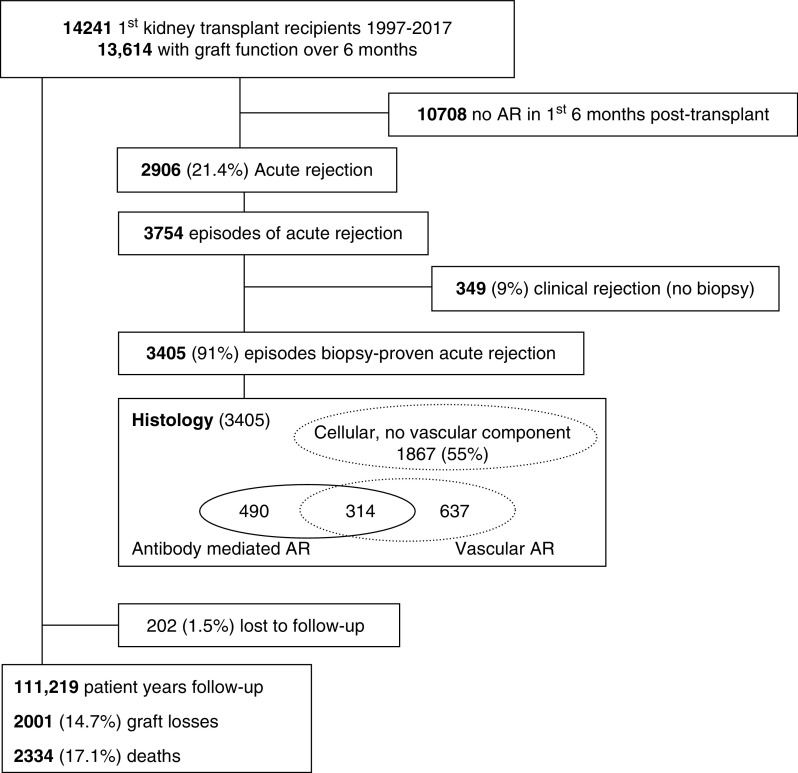
Methods: To understand the long-term effect of AR on outcomes, we analyzed data from the Australia and New Zealand Dialysis and Transplant Registry, including 13,614 recipients of a primary kidney-only transplant between 1997 and 2017 with at least 6 months of graft function. The associations between AR within 6 months post-transplant and subsequent cause-specific graft loss and death were determined using Cox models adjusted for baseline donor, recipient, and transplant characteristics.
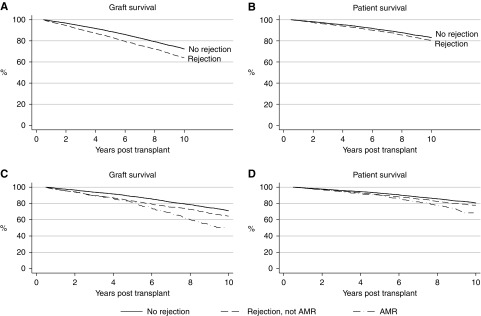
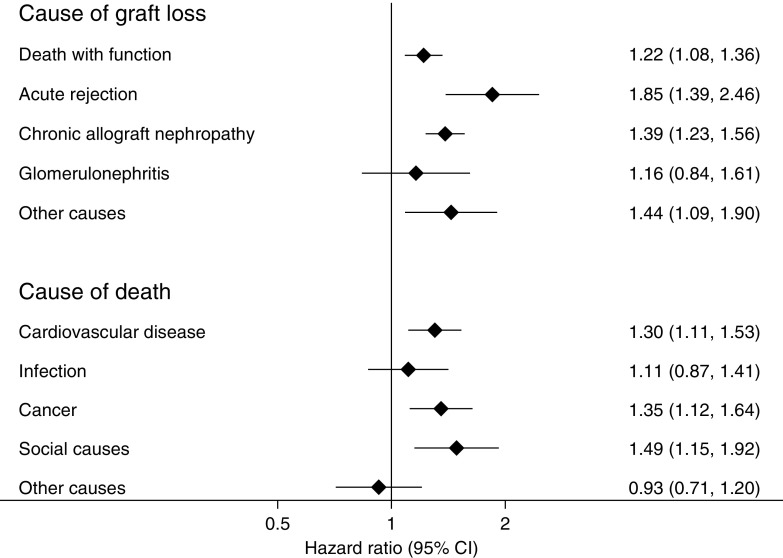
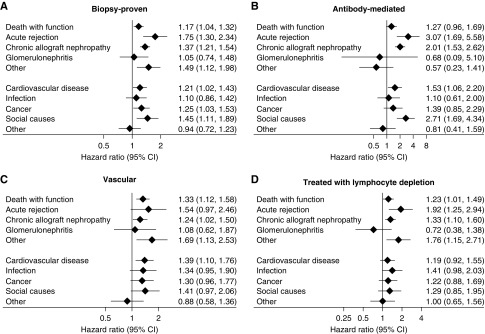
Results: AR occurred in 2906 recipients (21.4%) and was associated with graft loss attributed to chronic allograft nephropathy (hazard ratio [HR], 1.39; 95% confidence interval [95% CI], 1.23 to 1.56) and recurrent AR beyond month 6 (HR, 1.85; 95% CI, 1.39 to 2.46). Early AR was also associated with death with a functioning graft (HR, 1.22; 95% CI, 1.08 to 1.36), and with death due to cardiovascular disease (HR, 1.30; 95% CI, 1.11 to 1.53) and cancer (HR, 1.35; 95% CI, 1.12 to 1.64). Sensitivity analyses restricted to subgroups with either biopsy-proven, antibody-mediated, or vascular rejection, or stratified by treatment response produced similar results.
Conclusions: AR is associated with increased risks of longer-term graft failure and death, particularly death from cardiovascular disease and cancer. The results suggest AR remains an important short-term outcome to monitor in kidney transplantation and clinical trials.
Keywords: chronic allograft failure; kidney transplantation; rejection; survival.
Copyright © 2019 by the American Society of Nephrology.
Figures

References
-
- Organ Procurement and Transplantation Network (OPTN) and Scientific Registry of Transplant Recipients : (SRTR). OPTN/SRTR 2011 Annual Data Report, Rockville, MD, Department of Health and Human Services, Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation, 2012
-
- Australia and New Zealand Dialysis and Transplant Registry: 39th Annual Report, Chapter 8, Transplantation. Australia and New Zealand Dialysis and Transplant Registry, Adelaide, Australia, 2016
-
- McDonald S, Russ G, Campbell S, Chadban S: Kidney transplant rejection in Australia and New Zealand: Relationships between rejection and graft outcome. Am J Transplant 7: 1201–1208, 2007 - PubMed
-
- Meier-Kriesche HU, Schold JD, Srinivas TR, Kaplan B: Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am J Transplant 4: 378–383, 2004 - PubMed
-
- OʼConnell PJ, Kuypers DR, Mannon RB, Abecassis M, Chadban SJ, Gill JS, et al.: Clinical trials for immunosuppression in transplantation: The case for reform and change in direction. Transplantation 101: 1527–1534, 2017 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
