

Contribution of the uremic milieu to an increased pro-inflammatory monocytic phenotype in chronic kidney disease
- PMID: 31308443
- PMCID: PMC6629661
- DOI: 10.1038/s41598-019-46724-5
Contribution of the uremic milieu to an increased pro-inflammatory monocytic phenotype in chronic kidney disease
Abstract
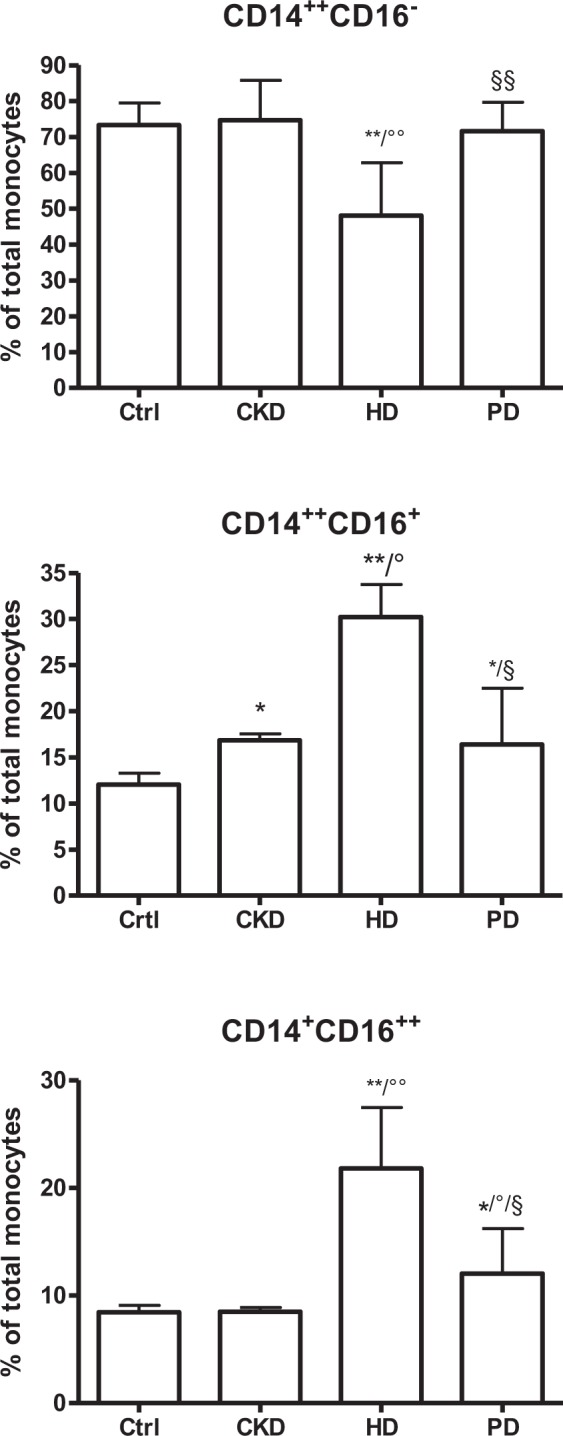
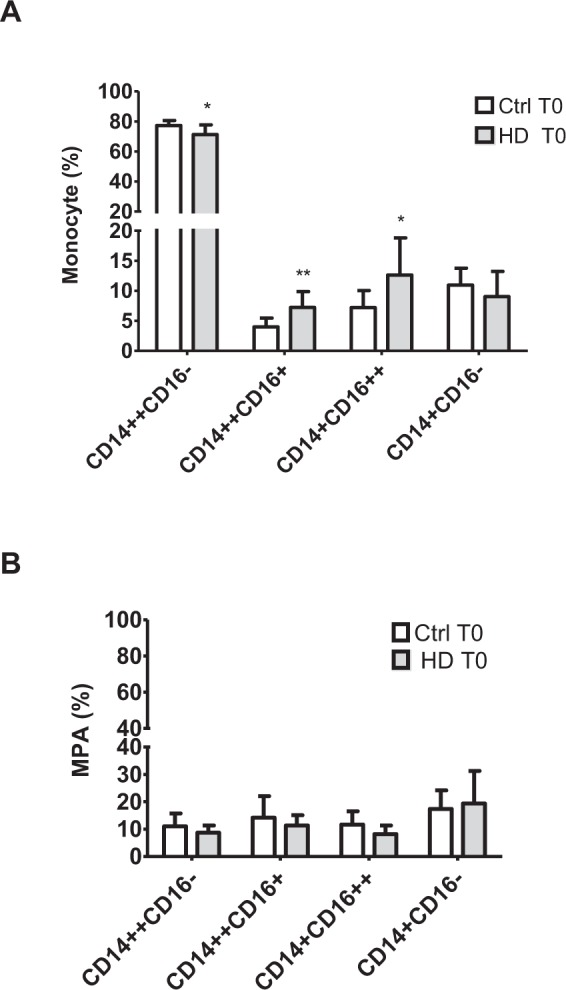
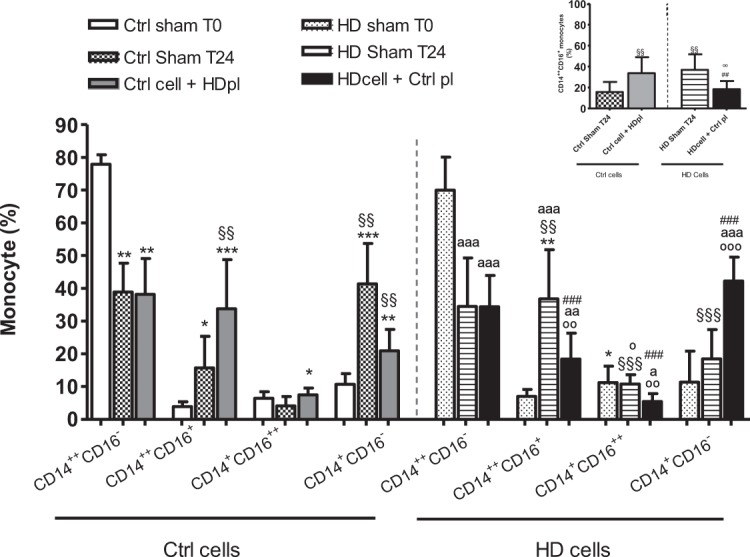
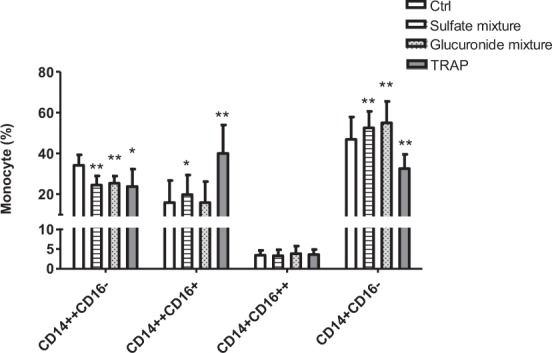
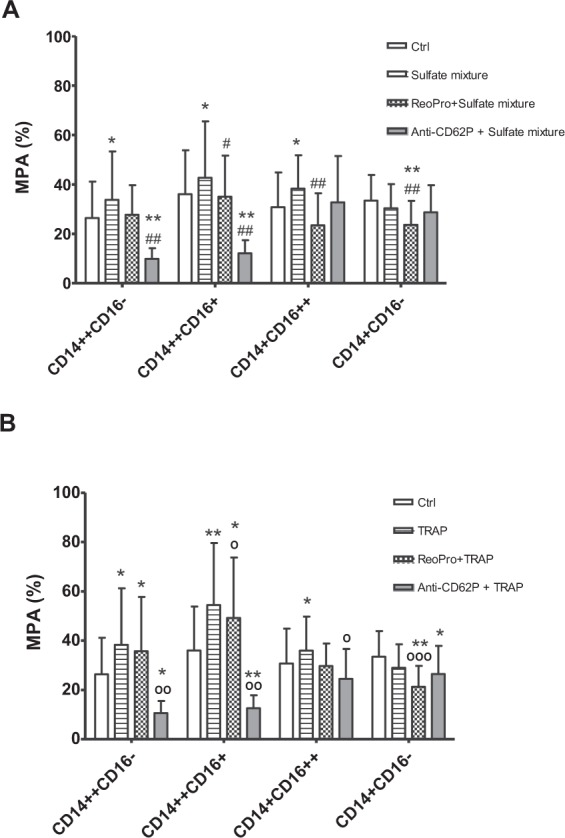
Intermediate (CD14++CD16+) monocytes have important pro-inflammatory and atherogenic features and are increased in patients with chronic kidney disease (CKD). The present study aims to elucidate the role of the uremic milieu and of platelet activation in monocyte differentiation. Monocyte subtypes were analyzed in CKD patients (n = 193) and healthy controls (n = 27). Blood from healthy controls (Ctrl; n = 8) and hemodialysis patients (HD; n = 8) was centrifuged, and plasma (pl) was exchanged between Ctrl and HD (Ctrlcells/HDpl and HDcells/Ctrlpl) or reconstituted as original (Ctrlsham and HDsham) and incubated for 24 h (T24). Monocyte differentiation and platelet aggregation to monocytes (MPA) was assessed by flow cytometry. Especially, a higher proportion of CD14++CD16+ monocytes was found in hemodialysis (HD) patients (p < 0.01). In plasma exchange experiments, Ctrl cells/HD pl T24 showed an increased percentage of CD14++CD16+ monocytes versus Ctrl sham (33.7% ± 15 vs. 15.7% ± 9.6; P < 0.005), comparable to the level of CD14++CD16+ monocytes in the HD sham condition. The percentage of CD14++CD16+ monocytes was lowered by suspending HD cells in Ctrl pl (18.4% ± 7.8 vs. 36.7% ± 15 in HD sham; P < 0.005) reaching the level of the Ctrl sham condition (15.7% ± 9.6). A mixture of uremic sulfates increased CD14++CD16+ monocytes compared to control (19.8 ± 9.6% vs. 15.8 ± 10.9%; P < 0.05), paralleled by a rise MPA. Blocking MPA by abciximab, a potential therapeutic strategy, or anti-CD62P did not inhibit differentiation towards the CD14++CD16+ monocytes. In conclusion, in the present cohort, CD14++CD16+ monocytes are especially increased in HD patients and this can at least in part be attributed to the presence of the uremic milieu, with uremic sulfates inducing a reversible shift towards pro-inflammatory CD14++CD16+ monocytes.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
