

Spotlight on emicizumab in the management of hemophilia A: patient selection and special considerations
- PMID: 31308776
- PMCID: PMC6613000
- DOI: 10.2147/JBM.S175952
Spotlight on emicizumab in the management of hemophilia A: patient selection and special considerations
Abstract
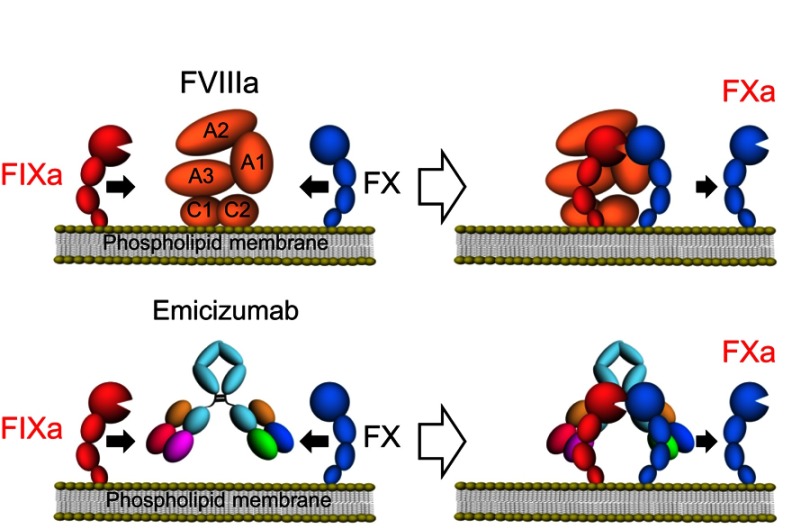
Emicizumab is a factor (F)VIIIa-mimicking bispecific antibody recognizing FIXa and FX molecules. In the phase 1/2 clinical studies, once-weekly subcutaneous administration of emicizumab has shown a favorable safety profile with encouraging efficacy in the patients with hemophilia A (PwHA) irrespective of the presence of anti-FVIII inhibitors. Moreover, in the following phase 3 studies, emicizumab treatment by once-weekly, bi-weekly or tetra-weekly administration have been still well-tolerated, but some thromboembolic events or thrombotic microangiopathy were observed associated with the concomitant use of activated prothrombin complex concentrates (aPCC) for breakthrough bleeds. Since approved for routine prophylaxis in PwHA in the US, EU, and Japan, a compass on patient selection for emicizumab treatment and special considerations on the practical situations such as concomitant treatment by bypassing agents (BPAs) or clotting factor concentrates (CFCs) with less thrombotic risk, inhibitor eradication by immune tolerance induction (ITI) should be provided. There is no doubt that emicizumab is an alternate first-line therapy for any existing BPA as hemostatic treatment for PwHA with inhibitor, but we should be more cautious in combination with aPCC on breakthrough bleeds under emicizumab prophylaxis because of thrombotic risk. For severe PwHA without inhibitor, since most patients are under CFCs prophylaxis, switching from CFCs to emicizumab should be considered when the advantage of emicizumab prophylaxis surpasses that of CFCs prophylaxis from the viewpoint of hemostatic effect by treatment, physical activity according to the life stage, health condition of the joints, adherence and complication. There are pros and cons on the timing of introduction of emicizumab for cases scheduled to start ITI or cases of ongoing ITI. Introduction of emicizumab to previously untreated patients and nonsevere PwHA without inhibitor is also required to discuss in consideration of risk of inhibitor development and unforeseen safety issues.
Keywords: bypassing agent; emicizumab; hemophilia; inhibitor; noninhibitor.
Conflict of interest statement
KN is an inventor of the patents relating to emicizumab. KY and KN are engaged in clinical studies sponsored by Chugai and F. Hoffmann-La Roche. KY teaches a course endowed by Shire Japan Co. Ltd. KY also reports nonfinancial support from Chugai Pharmaceutical, F. Hoffmann-La Roche, and Shire Japan Co. Ltd., during the conduct of the study. KN reports grants and personal fees, from Shire, Japan Co. Ltd., Novo Nordisk, Bioverativ, and Bayer, during the conduct of the study. KN also receives personal fees from Chugai Pharmaceutical. In addition, KN has a patent pending with Chugai. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
[Emicizumab, a bispecific antibody mimicking factor VIII: a novel alternative therapy for hemophilia A with inhibitors].Rinsho Ketsueki. 2019;60(5):475-479. doi: 10.11406/rinketsu.60.475. Rinsho Ketsueki. 2019. PMID: 31168016 Japanese.
-
Efficacy, safety, and pharmacokinetics of emicizumab prophylaxis given every 4 weeks in people with haemophilia A (HAVEN 4): a multicentre, open-label, non-randomised phase 3 study.Lancet Haematol. 2019 Jun;6(6):e295-e305. doi: 10.1016/S2352-3026(19)30054-7. Epub 2019 Apr 16. Lancet Haematol. 2019. PMID: 31003963 Clinical Trial.
-
Economic impact model of delayed inhibitor development in patients with hemophilia a receiving emicizumab for the prevention of bleeding events.J Med Econ. 2019 Dec;22(12):1328-1337. doi: 10.1080/13696998.2019.1669614. Epub 2019 Oct 7. J Med Econ. 2019. PMID: 31530050
-
Key questions in the new hemophilia era: update on concomitant use of FVIII and emicizumab in hemophilia A patients with inhibitors.Expert Rev Hematol. 2021 Feb;14(2):143-148. doi: 10.1080/17474086.2021.1875817. Epub 2021 Jan 27. Expert Rev Hematol. 2021. PMID: 33499681 Review.
-
Clinical pharmacology of emicizumab for the treatment of hemophilia A.Expert Rev Clin Pharmacol. 2023 Jul-Dec;16(9):775-790. doi: 10.1080/17512433.2023.2243213. Epub 2023 Aug 21. Expert Rev Clin Pharmacol. 2023. PMID: 37529848 Review.
Cited by
-
Design of an international investigator-initiated study on MOdern Treatment of Inhibitor-positiVe pATiEnts with haemophilia A (MOTIVATE).Ther Adv Hematol. 2021 Sep 23;12:20406207211032452. doi: 10.1177/20406207211032452. eCollection 2021. Ther Adv Hematol. 2021. PMID: 34589194 Free PMC article.
-
Fc Gamma Receptors and Complement Component 3 Facilitate Anti-fVIII Antibody Formation.Front Immunol. 2020 Jun 9;11:905. doi: 10.3389/fimmu.2020.00905. eCollection 2020. Front Immunol. 2020. PMID: 32582142 Free PMC article.
-
Translational Potential of Immune Tolerance Induction by AAV Liver-Directed Factor VIII Gene Therapy for Hemophilia A.Front Immunol. 2020 Apr 28;11:618. doi: 10.3389/fimmu.2020.00618. eCollection 2020. Front Immunol. 2020. PMID: 32425925 Free PMC article. Review.
-
Engineering a Therapeutic Protein to Enhance the Study of Anti-Drug Immunity.Biomedicines. 2022 Jul 18;10(7):1724. doi: 10.3390/biomedicines10071724. Biomedicines. 2022. PMID: 35885029 Free PMC article.
-
Concomitant use of bypassing agents with emicizumab for people with haemophilia A and inhibitors undergoing surgery.Haemophilia. 2021 Jul;27(4):519-530. doi: 10.1111/hae.14322. Epub 2021 May 14. Haemophilia. 2021. PMID: 33988293 Free PMC article. Review.
References
-
- White GC II, Rosendaal F, Aledort LM, Lusher JM, Rothschild C, Ingerslev J. Definitions in hemophilia: recommendation of the scientific subcommittee on factor VIII and factor IX of the scientific and standardization committee of the International Society on Thrombosis and Haemostasis. Thromb Haemost. 2001;85(3):560. doi:10.1055/s-0037-1615621 - DOI - PubMed
-
- Luck JV Jr, Silva M, Rodriguez-Merchan EC, Ghalambor N, Zahiri CA, Finn RS. Hemophilic arthropathy. J Am Acad Orthop Surg. 2004;12(4):234–245. - PubMed
-
- Nilsson IM, Hedner U, Ahlberg A. Hemophilia prophylaxis in Sweden. Acta Paediatr Scand. 1976;65(2):129–135. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
