

Uterine sarcoma: a clinical case and a literature review
- PMID: 31308826
- PMCID: PMC6591694
- DOI: 10.6001/actamedica.v25i4.3931
Uterine sarcoma: a clinical case and a literature review
Abstract
Background: Uterine sarcomas are rare gynaecologic tumours representing 3-7% of all uterine malignancies. The aetiology of sarcomas is still unclear: it is thought, that chromosomal translocations have influence on wide histological variety of sarcomas. Presenting symptoms are vague and nonspecific. Usually sarcoma causes abnormal vaginal bleeding, can cause abdominal or pelvic pain, or manifests as a rapidly growing uterine tumour. The diagnosis of sarcoma is often made retrospectively after surgical removal of a presumed benign uterine neoplasm, because imaging modalities such as ultrasound, computed tomography, or magnetic resonance imaging cannot yet accurately and reliably distinguish between benign leiomyoma and malignant pathology. If there are certain clinical features that raise a suspicion of malignancy in the uterus, it is recommended to avoid the use of power morcellation through laparoscopic surgery in order to prevent disease dissemination.
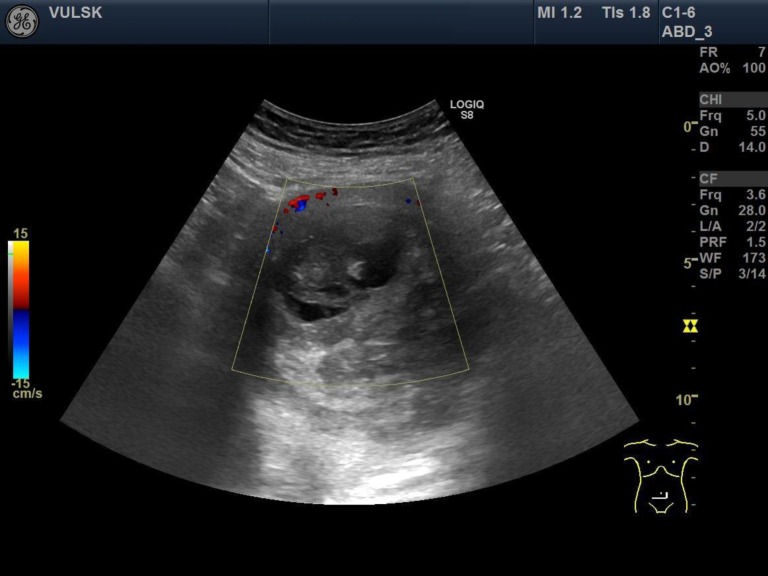
Materials and methods: We present a clinical case of a 64-year-old patient, who was referred to hospital due to abdominal pain and tenesmus that lasted for two days. From a past medical history it was known that previously the patient had been diagnosed with uterine myoma. Transvaginal ultrasonography showed a 10.4 cm × 9.8 cm uterine tumour of nonhomogeneous structure with signs of necrosis and good vascularization. The patient refused urgent hysterectomy, that was advised to her. The patient was operated on one month later and total hysterectomy with bilateral salpingooforectomy was performed. Postoperative histological evaluation showed undifferentiated sarcoma uterus pT1b L/V0. Imaging modalities were made to evaluate possible dissemination of the disease. In the absence of signs of disease progression, the patient received radiotherapy and brachytherapy and was followed-up by doctors.
Results and conclusions: Uterine sarcomas are highly malignant tumours that originate from smooth muscles and connective tissue elements of the uterus and make up 1% of all malignant gynaecological tumours and about 3-7% of all malignant uterine tumours. Imaging modalities cannot yet reliably distinguish benign myomas from malignant sarcomas. It is important not to damage the wholeness of uterus during operation in order to prevent dissemination of the disease in the abdominal cavity. The low-grade endometrial stromal sarcoma has the best survival prognosis, while carcinosarcoma and undifferentiated uterine sarcoma have the lowest survival rates.
SantraukaTikslas. Gimdos sarkomos yra reti ginekologiniai navikai, sudarantys 3–7 % visų piktybinių gimdos navikų. Sarkomų atsiradimo etiologija nėra aiški, manoma, kad įtakos tam turi skirtingos genų ir chromosomų mutacijos, lemiančios didelę sarkomų histologinę įvairovę. Simptomatika nėra specifiška tik sarkomoms, šie navikai dažniausiai sukelia nenormalius kraujavimus iš gimdos, neaiškius pilvo ir dubens skausmus ar gali pasireikšti greitu gimdos darinio augimu. Diagnozė dažniausiai nustatoma po operacijos, pašalinus iki tol gerybiniu laikytą gimdos darinį ir ištyrus histologiškai, nes ikioperaciniai vaizdiniai tyrimai negali patikimai atskirti gerybinių gimdos lejomiomų nuo piktybinių sarkomų. Jeigu tiriant pastebimi požymiai, kad gali būti gimdos sarkoma, reikėtų vengti tokias pacientes operuoti naudojant morceliatorių operaciniams dariniams smulkinti, nes kyla grėsmė, kad piktybiniai dariniai išsisės pilvo ertmėje. Straipsnio tikslas – konkretaus klinikinio atvejo pavyzdžiu aprašyti diagnostikos ir gydymo metodus nustačius gimdos naviką moteriai po menopauzės.Medžiaga ir metodai. Pristatome 64 metų pacientės klinikinį atvejį, kuri atvyko į ligoninę dėl dvi paras besitęsiančių pilvo skausmų ir pasunkėjusio tuštinimosi. Iš anamnezės buvo žinoma, kad pacientei prieš penkerius metus ambulatoriškai diagnozuota gimdos mioma. Ultragarsiniu tyrimu per makštį pacientei nustatyta 10,4 × 9,8 cm dydžio nehomogeniškos struktūros su nekrozės požymiais, gerai vaskuliarizuota gimdos intramuralinė mioma. Ligonei dėl pilvo skausmų buvo rekomenduotas operacinis gydymas skubos tvarka, įtariant miomos mazgo nekrozę, tačiau moteris atsisakė skubios operacijos. Rekomendavus operacinį gydymą planine tvarka ir paskyrus ambulatorinį ištyrimą bei gydymą, pacientė išvyko į namus. Po vieno mėnesio ligonei buvo atlikta planinė operacija – totalinė histerektomija su abipusiais gimdos priedais. Ištyrus gimdą histologiškai buvo diagnozuota nediferencijuota gimdos sarkoma pT1b L/V0. Kadangi vaizdinių tyrimai nerodė ligos išplitimo, pacientei buvo paskirta adjuvantinė spindulinė terapija ir endovagininė brachiterapija bei rekomenduotas tolimesnis stebėjimas.Rezultatai ir išvados. Gimdos sarkoma yra didelio piktybiškumo navikas, augantis iš gimdos lygiųjų raumenų bei jungiamojo audinio, sudarantis 1 % visų piktybinių ginekologinių navikų ir apie 3–7 % visų piktybinių gimdos navikų. Vaizdiniais tyrimais negalima patikimai atskirti gerybinių gimdos miomų nuo piktybinių gimdos sarkomų. Labai svarbu operuojant ligonę, kuriai diagnozuotas gimdos navikas, nepažeisti gimdos sienelės vientisumo norint išvengti patologinio proceso išplitimo į pilvo ertmę. Mažo laipsnio endometriumo stromos sarkomos atveju ligonių išgyvenamumo prognozė yra geriausia, o karcinosarkomos ir nediferencijuotos gimdos sarkomos atvejais – blogiausia.Raktažodžiai: gimdos tumoras, piktybinė gimdos neoplazija, gimdos sarkoma, nediferencijuota gimdos sarkoma, gimdos sarkomos diagnostika ir gydymas.
Keywords: malignant uterine neoplasm; treatment; undifferentiated uterine sarcoma; uterine sarcoma; uterine sarcoma diagnosis; uterine tumour.
Figures

Similar articles
-
[Uterine sarcomas: clinical and histopathological aspects. Report on 15 cases].Gynecol Obstet Fertil. 2008 Jun;36(6):628-35. doi: 10.1016/j.gyobfe.2008.03.012. Epub 2008 Jun 5. Gynecol Obstet Fertil. 2008. PMID: 18538624 French.
-
A High-Grade Undifferentiated Endometrial Stromal Sarcoma Presenting as Inversion of the Uterus: A Rare Case.J Midlife Health. 2020 Jan-Mar;11(1):40-44. doi: 10.4103/jmh.JMH_75_19. Epub 2020 May 4. J Midlife Health. 2020. PMID: 32684727 Free PMC article.
-
In-bag manual versus uncontained power morcellation for laparoscopic myomectomy.Cochrane Database Syst Rev. 2020 May 6;5(5):CD013352. doi: 10.1002/14651858.CD013352.pub2. Cochrane Database Syst Rev. 2020. PMID: 32374421 Free PMC article.
-
Diagnosis and surgical therapy of uterine sarcoma.Acta Chir Iugosl. 2006;53(3):67-72. doi: 10.2298/aci0603067v. Acta Chir Iugosl. 2006. PMID: 17338203
-
The management of patients with uterine sarcoma: a debated clinical challenge.Crit Rev Oncol Hematol. 2008 Feb;65(2):129-42. doi: 10.1016/j.critrevonc.2007.06.011. Epub 2007 Aug 13. Crit Rev Oncol Hematol. 2008. PMID: 17706430 Review.
Cited by
-
The role of extracellular vesicles in the pathogenesis of gynecological cancer.Front Oncol. 2024 Sep 26;14:1477610. doi: 10.3389/fonc.2024.1477610. eCollection 2024. Front Oncol. 2024. PMID: 39391238 Free PMC article. Review.
-
An enormous pelvic tumor in a 46-year-old woman with an elevated serum CA 125 level, what lies beneath it? Investigation of uterine tumors in postmenopausal women.Prz Menopauzalny. 2021 Sep;20(3):154-157. doi: 10.5114/pm.2021.109773. Epub 2021 Oct 11. Prz Menopauzalny. 2021. PMID: 34703417 Free PMC article.
-
Adjuvant radiotherapy shows benefit in selected stage I uterine sarcoma: A risk scoring system based on a population analysis.Cancer Med. 2022 Jul;11(14):2846-2854. doi: 10.1002/cam4.4643. Epub 2022 Mar 11. Cancer Med. 2022. PMID: 35277934 Free PMC article.
-
Lipoleiomyosarcoma with pleomorphic liposarcoma of the uterus: Computed tomography findings with pathological correlation. A case report and review of literature.Radiol Case Rep. 2024 Sep 3;19(11):5474-5480. doi: 10.1016/j.radcr.2024.08.004. eCollection 2024 Nov. Radiol Case Rep. 2024. PMID: 39285970 Free PMC article.
-
Uterine carcinosarcoma with intestinal involvement: A case report and literature review.Med Int (Lond). 2023 Mar 1;3(2):15. doi: 10.3892/mi.2023.75. eCollection 2023 Mar-Apr. Med Int (Lond). 2023. PMID: 36925759 Free PMC article.
References
-
- Seagle B-LL, Sobecki-Rausch J, Strohl AE, Shilpi A, Grace A, Shahabi S. Prognosis and treatment of uterine leiomyosarcoma: a National Cancer Database study. Gynecol Oncol. 2017. April; 145(1): 61–70. - PubMed
-
- Hosh M, Antar S, Nazzal A, Warda M, Gibreel A, Refky B. Uterine sarcoma: analysis of 13,089 cases based on surveillance, epidemiology, and end results database. Int J Gynecol Cancer. 2016. July; 26(6): 1098–104. - PubMed
-
- Gockley AA, Rauh-Hain JA, del Carmen MG. Uterine leiomyosarcoma: a review article. Int J Gynecol Cancer. 2014. November; 24(9): 1538–42. - PubMed
-
- Ryan GL, Syrop CH, Van Voorhis BJ. Role, epidemiology, and natural history of benign uterine mass lesions. Clin Obstet Gynecol. 2005. June; 48(2): 312–24. - PubMed
-
- Sivakumari S, Rajaraman R, Subbiah S. Uterine sarcoma: the Indian scenario. Indian J Surg Oncol [Internet]. 2015. September 14; 6(3): 232–6. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4856672/ - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous