

Differential left ventricular and left atrial remodelling in heart failure with preserved ejection fraction patients with and without diabetes
- PMID: 31308926
- PMCID: PMC6613057
- DOI: 10.1177/2042018819861593
Differential left ventricular and left atrial remodelling in heart failure with preserved ejection fraction patients with and without diabetes
Abstract
Background: Attempts to characterize cardiac structure in heart failure with preserved ejection fraction (HFpEF) in people with type 2 diabetes (T2D) have yielded inconsistent findings. We aimed to determine whether patients with HFpEF and T2D have a distinct pattern of cardiac remodelling compared with those without diabetes and whether remodelling was related to circulating markers of inflammation and fibrosis and clinical outcomes.
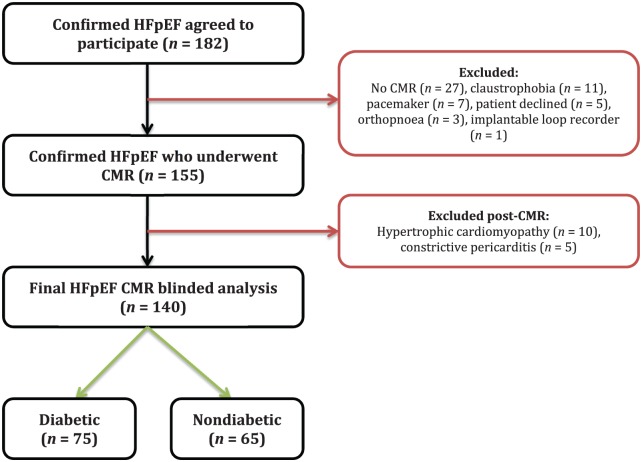
Methods: We recruited 140 patients with HFpEF (75 with T2D and 65 without). Participants underwent comprehensive cardiovascular phenotyping, including echocardiography, cardiac magnetic resonance imaging and plasma biomarker profiling.
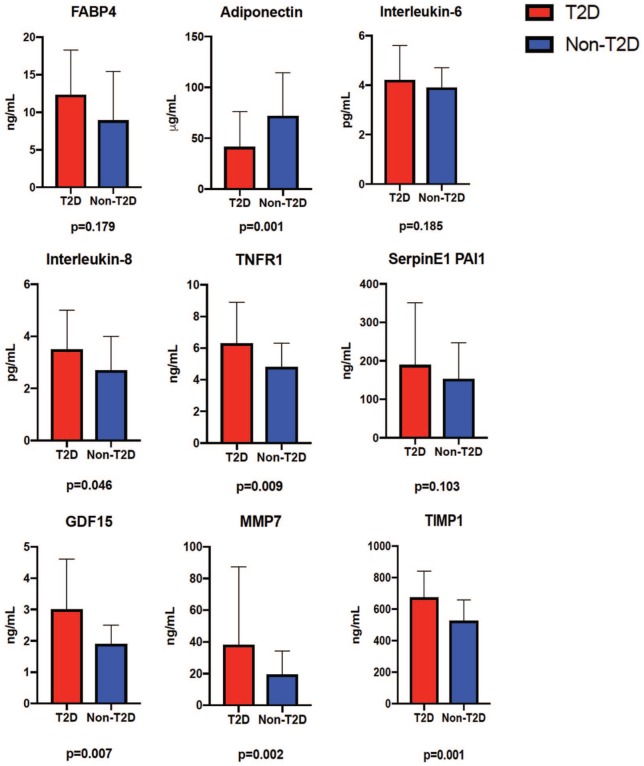
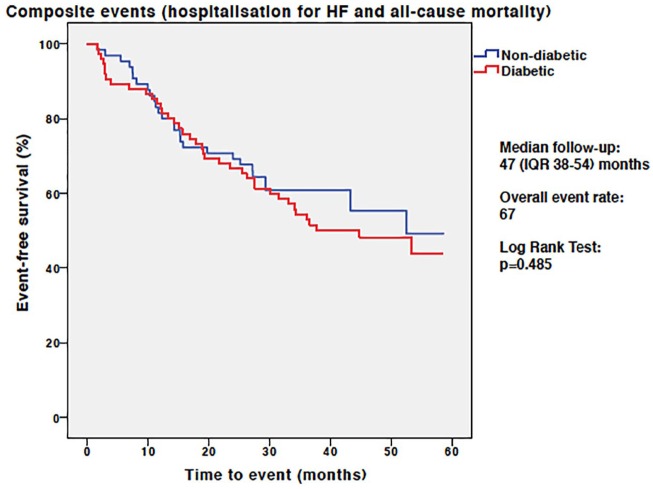
Results: Patients with T2D were younger (age 70 ± 9 versus 75 ± 9y, p = 0.002), with evidence of more left ventricular (LV) concentric remodelling (LV mass/volume ratio 0.72 ± 0.15 versus 0.62 ± 0.16, p = 0.024) and smaller indexed left atrial (LA) volumes (maximal LA volume index 48 ± 20 versus 59 ± 29 ml/m2, p = 0.004) than those without diabetes. Plasma biomarkers of inflammation and extracellular matrix remodelling were elevated in those with T2D. Overall, there were 45 hospitalizations for HF and 22 deaths over a median follow-up period of 47 months [interquartile range (IQR) 38-54]. There was no difference in the primary composite endpoint of hospitalization for HF and mortality between groups. On multivariable Cox regression analysis, age, prior HF hospitalization, history of pulmonary disease and LV mass/volume were independent predictors of the primary endpoint.
Conclusions: Patients with HFpEF and T2D have increased concentric LV remodelling, smaller LA volumes and evidence of increased systemic inflammation compared with those without diabetes. This suggests the underlying pathophysiology for the development of HFpEF is different in patients with and without T2D.
Clinicaltrialsgov identifier: NCT03050593.
Keywords: cardiovascular magnetic resonance imaging; heart failure with preserved ejection fraction; type 2 diabetes mellitus.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
References
-
- Dunlay SM, Roger VL, Redfield MM. Epidemiology of heart failure with preserved ejection fraction. Nat Rev Cardiol 2017; 14: 591–602. - PubMed
-
- Owan TE, Hodge DO, Herges RM, et al. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006; 355: 251–259. - PubMed
-
- Komajda M, Lam CS. Heart failure with preserved ejection fraction: a clinical dilemma. Eur Heart J 2014; 35: 1022–1032. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
