

Alcohol use disorders and the heart
- PMID: 31309639
- PMCID: PMC6771559
- DOI: 10.1111/add.14703
Alcohol use disorders and the heart
Abstract
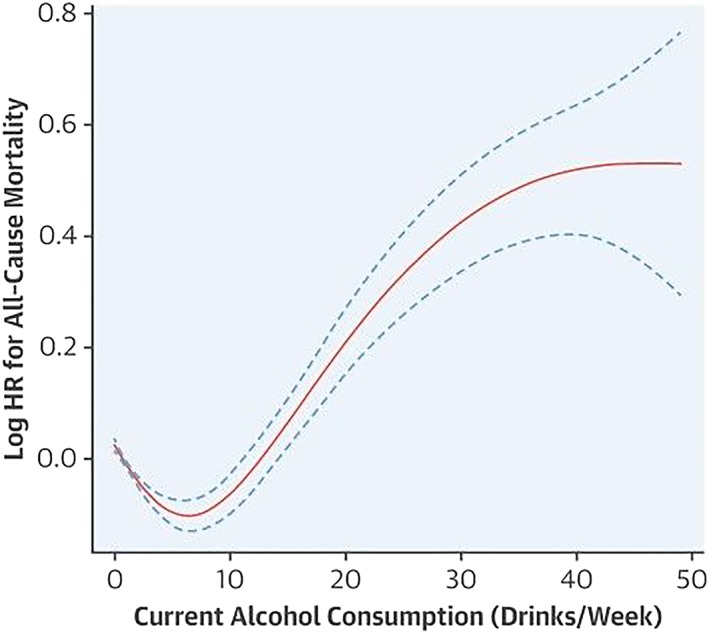
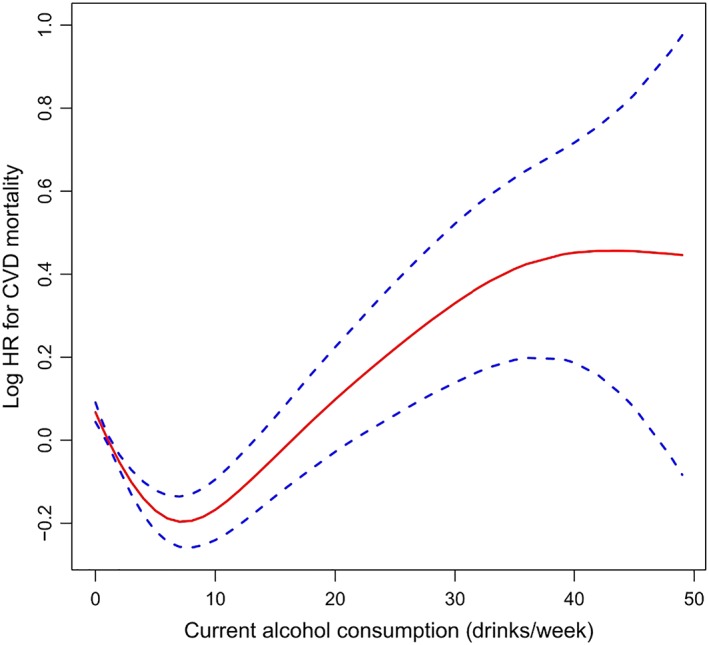
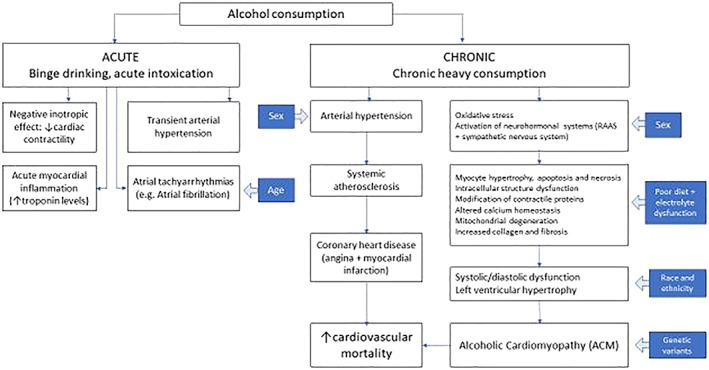
Alcohol use is an important preventable and modifiable cause of non-communicable disease, and has complex effects on the cardiovascular system that vary with dose. Observational and prospective studies have consistently shown a lower risk of cardiovascular and all-cause mortality in people with low levels of alcohol consumption when compared to abstainers (the 'J'-shaped curve). Maximum potential benefit occurs at 0.5 to one standard drinks (7-14 g pure ethanol) per day for women (18% lower all-cause mortality, 95% confidence interval (CI) = 13-22%) and one to two standard drinks (14-28 g ethanol) per day for men (17% lower all-cause mortality, 95% CI = 15-19%). However, this evidence is contested, and overall the detrimental effects of alcohol far outweigh the beneficial effects, with the risk of premature mortality increasing steadily after an average consumption of 10 g ethanol/day. Blood pressure (BP) is increased by regular alcohol consumption in a dose-dependent manner, with a relative risk for hypertension (systolic BP > 140 mm Hg or diastolic > 90 mm Hg) of 1.7 for 50 g ethanol/day and 2.5 at 100 g/day. Important reductions in BP readings can be expected after as little as 1 month of abstinence from alcohol. Heavy alcohol consumption in a binge pattern is associated with the development of acute cardiac arrhythmia, even in people with normal heart function. Atrial fibrillation is the most common arrhythmia associated with chronic high-volume alcohol intake, and above 14 g alcohol/day the relative risk increases 10% for every extra standard drink (14 g ethanol). Ethanol and its metabolites have toxic effects on cardiac myocytes, and alcoholic cardiomyopathy (ACM) accounts for a third of all cases of non-ischaemic dilated cardiomyopathy. Screening people drinking alcohol above low-volume levels and delivering a brief intervention may prevent the development of cardiovascular complications. Although people with established cardiovascular disease show improved outcomes with a reduction to low-volume alcohol consumption, there is no safe amount of alcohol to drink and patients with ACM should aim for abstinence in order to optimize medical treatment.
Keywords: Alcohol; arrhythmia; cardiac; cardiomyopathy; cardiovascular; hypertension; mortality.
© 2019 The Authors. Addiction published by John Wiley & Sons Ltd on behalf of Society for the Study of Addiction.
Figures
References
-
- Meister P. Mythology in Pathology? The Munich Beer Heart Revisited: United States and Canadian Academy of Pathology; 2003. Available at: http://uscapknowledgehub.org/index.htm?92nd/companion09h3.htm (accessed 16 June 2019).
-
- World Health Organization (WHO) Global Status Report on Alcohol and Health 2014. Geneva: WHO Press; 2014.
-
- Rehm J., Mathers C., Popova S., Thavorncharoensap M., Teerawattananon Y., Patra J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol‐use disorders. Lancet 2009; 373: 2223–2233. - PubMed
-
- Global Burden of Disease Study (GBD) 2016 Alcohol Collaborators , Griswold M. G., Fullman N., Hawley C., Arian N., Zimsen S. R. M., et al Alcohol use and burden for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018; 392: 1015–1035. - PMC - PubMed
-
- Xi B., Veeranki S. P., Zhao M., Ma C., Yan Y., Mi J. Relationship of alcohol consumption to all‐cause, cardiovascular, and cancer‐related mortality in U.S. adults. J Am Coll Cardiol 2017; 70: 913–922. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
