

Hospitalization Risk among Older Adults with Chronic Kidney Disease
- PMID: 31311014
- PMCID: PMC6726535
- DOI: 10.1159/000501539
Hospitalization Risk among Older Adults with Chronic Kidney Disease
Abstract
Introduction: Chronic kidney disease (CKD) risk staging is based on estimated glomerular filtration rate (eGFR) and albumin-creatinine ratio (ACR). However, the relationship between all-cause hospitalization risk and the current CKD staging system has not been well studied among older adults, despite a high prevalence of CKD and a high risk of hospitalization in old age.
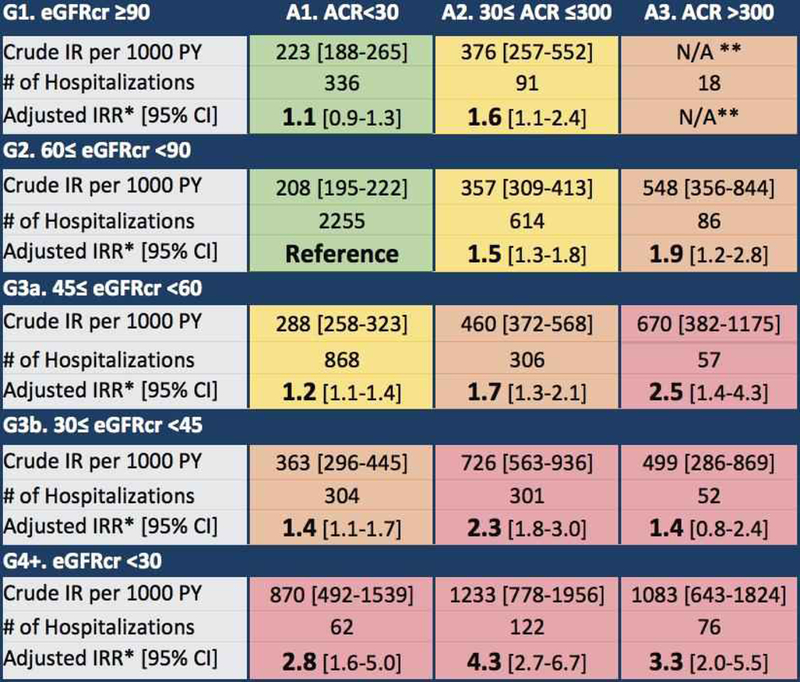
Methods: Among 4,766 participants of the Atherosclerosis Risk in Communities study, CKD was staged according to Kidney Disease Improving Global Outcomes (KDIGO) criteria, using creatinine-based eGFR (eGFRcr) and ACR. Incidence rates of all-cause hospitalization associated with each CKD risk group were analyzed using negative binomial regression. Additionally, cause-specific hospitalization risks for cardiovascular, infectious, kidney, and other diseases were estimated. The impacts of using cystatin C-based eGFR (eGFRcys) to estimate the prevalence of CKD and risks of hospitalization were also quantified.
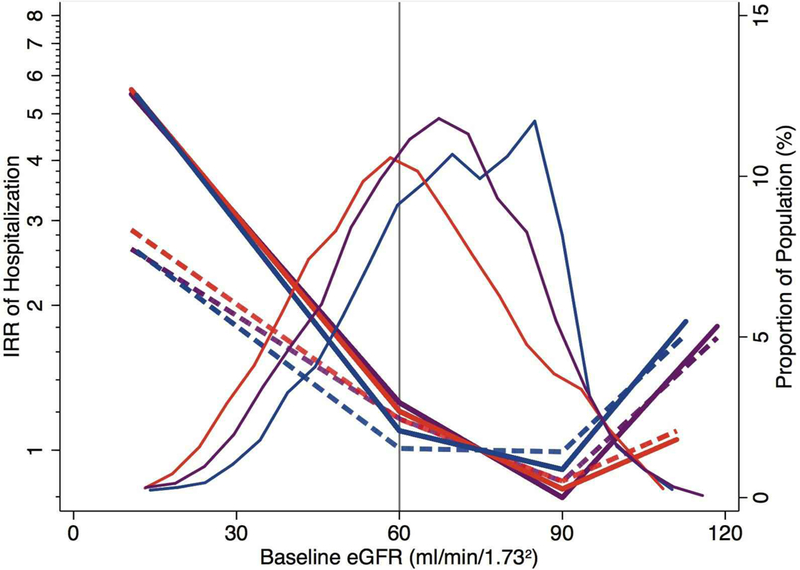
Results: Participants experienced 5,548 hospitalizations and 29% had CKD. Hospitalization rates per 1,000 person-years according to KDIGO risk categories were 208-223 ("low risk"), 288-376 ("moderately increased risk"), 363-548 ("high risk"), and 499-1083 ("very high risk"). The increased risk associated with low eGFR and high ACR persisted in adjusted analyses, examinations of cause-specific hospitalizations, and when CKD was staged by eGFRcys or eGFRcr-cys, a combined equation based on both creatinine and cystatin C. In comparison to eGFRcr, staging by eGFRcys increased the prevalence of CKD to 50%, but hospitalization risks remained similarly high.
Discussion/conclusion: In older adults, decreased eGFR, increased ACR, and KDIGO risk stages based on a combination of these measures, were strong risk factors for hospitalization. These relationships were consistent, regardless of the marker used to estimate GFR, but the use of cystatin C resulted in a substantially higher prevalence of CKD than the use of creatinine. Older adults in the population with very high risk stages of CKD have hospitalization rates exceeding 500 per 1,000 person-years.
Keywords: Aging; Albuminuria; Chronic kidney disease; Estimated glomerular filtration rate; Hospitalization.
© 2019 S. Karger AG, Basel.
Conflict of interest statement
Disclosure Statement
The authors have no conflicts of interest to declare. Abstracts of interim findings were presented at the American Heart Association’s EPI Lifestyle Scientific Sessions 2018 and the Society of Epidemiologic Research 2018 Annual Meeting.
Figures
References
-
- Manjunath G, Tighiouart H, Coresh J, Macleod B, Salem DN, Griffith JL, et al. Level of kidney function as a risk factor for cardiovascular outcomes in the elderly. Kidney Int. 2003;63(3):1121–9. - PubMed
-
- Shlipak MG, Sarnak MJ, Katz R, Fried LF, Seliger SL, Newman AB, et al. Cystatin C and the risk of death and cardiovascular events among elderly persons. The New England journal of medicine. 2005;352(20):2049–60. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K01 DK107782/DK/NIDDK NIH HHS/United States
- R21 HL143089/HL/NHLBI NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- HHSN268201700002C/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- HHSN268201700004C/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
