

Haemostatic Changes in Five Patients Infected with Ebola Virus
- PMID: 31311112
- PMCID: PMC6669445
- DOI: 10.3390/v11070647
Haemostatic Changes in Five Patients Infected with Ebola Virus
Abstract
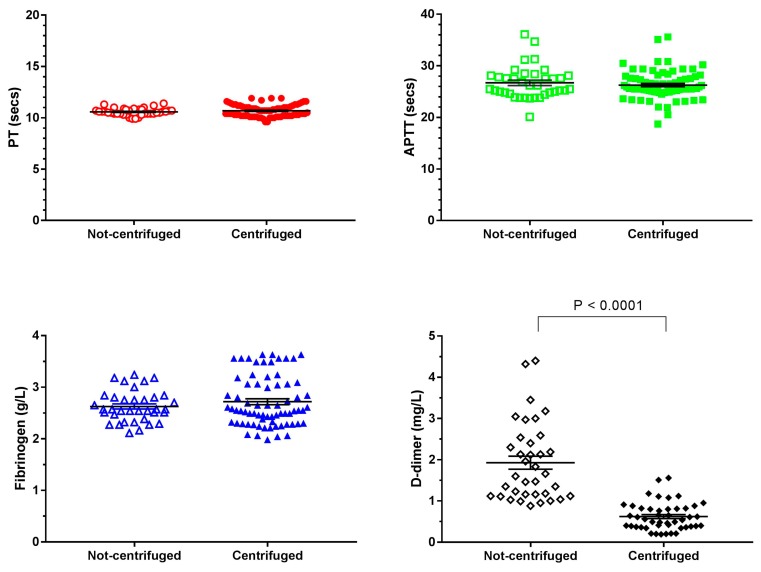
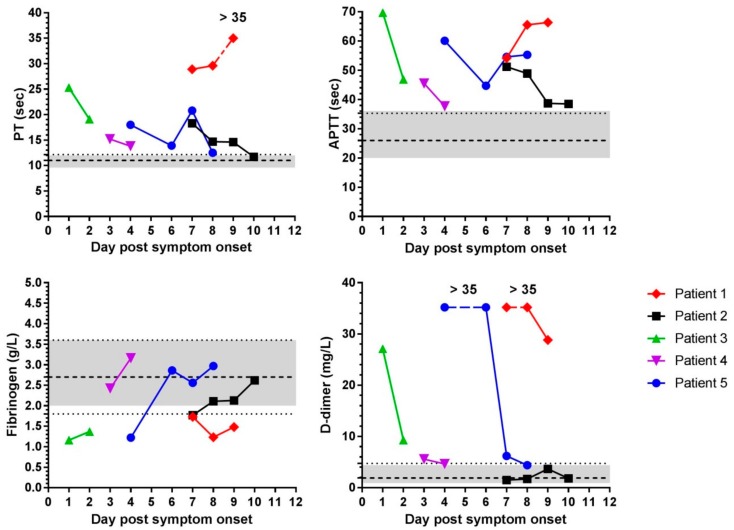
Knowledge on haemostatic changes in humans infected with Ebola virus is limited due to safety concerns and access to patient samples. Ethical approval was obtained to collect plasma samples from patients in Sierra Leone infected with Ebola virus over time and samples were analysed for clotting time, fibrinogen, and D-dimer levels. Plasma from healthy volunteers was also collected by two methods to determine effect of centrifugation on test results as blood collected in Sierra Leone was not centrifuged. Collecting plasma without centrifugation only affected D-dimer values. Patients with Ebola virus disease had higher PT and APTT and D-dimer values than healthy humans with plasma collected in the same manner. Fibrinogen levels in patients with Ebola virus disease were normal or lower than values measured in healthy people. Clotting times and D-dimer levels were elevated during infection with Ebola virus but return to normal over time in patients that survived and therefore could be considered prognostic. Informative data can be obtained from plasma collected without centrifugation which could improve patient monitoring in hazardous environments.
Keywords: APTT; D-dimers; Ebola virus; PT; clotting; fibrinogen; haemostasis.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Nyakarahuka L., Kankya C., Krontveit R., Mayer B., Mwiine F.N., Lutwama J., Skjerve E. How severe and prevalent are Ebola and Marburg viruses? A systematic review and meta-analysis of the case fatality rates and seroprevalence. BMC Infect. Dis. 2016;16:708. doi: 10.1186/s12879-016-2045-6. - DOI - PMC - PubMed
-
- Centers for Disease Control and Prevention (CDC) Guidance for U.S. Laboratories for Managing and Testing Routine Clinical Specimens When There Is a Concern about Ebola Virus Disease. [(accessed on 23 April 2019)]; Available online: http://www.cdc.gov/vhf/ebola/healthcare-us/laboratories/safe-specimen-ma....
-
- Hunt L., Gupta-Wright A., Simms V., Tamba F., Knott V., Tamba K., Heisenberg-Mansaray S., Tamba E., Sheriff A., Conteh S. Clinical presentation, biochemical, and haematological parameters and their association with outcome in patients with Ebola virus disease: An observational cohort study. Lancet Infect. Dis. 2015;15:1292–1299. doi: 10.1016/S1473-3099(15)00144-9. - DOI - PubMed
-
- Isaacson M., Sureau P., Courteille G., Pattyn S.R. Clinical aspects of Ebola virus disease at the Ngaliema hospital, Kinshasa, Zaire, 1976. In: Pattyn S.R., editor. Ebola Virus Haemorrhagic Fever. Elsevier/North-Holland Biomedical Press; New York, NY, USA: 1978. pp. 15–20.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
