

Comparison of medical outcomes and health care costs at the end of life between dialysis patients with and without cancer: a national population-based study
- PMID: 31311518
- PMCID: PMC6636130
- DOI: 10.1186/s12882-019-1440-9
Comparison of medical outcomes and health care costs at the end of life between dialysis patients with and without cancer: a national population-based study
Abstract
Background: Palliative care has improved the quality of end-of-life (EOL) care and lowered the health care cost of cancer, and these benefits should be extended to patients with other serious illnesses including end-stage kidney disease. We evaluated the quality of EOL care, survival probabilities, and health care costs for dialysis patients in their last month of life.
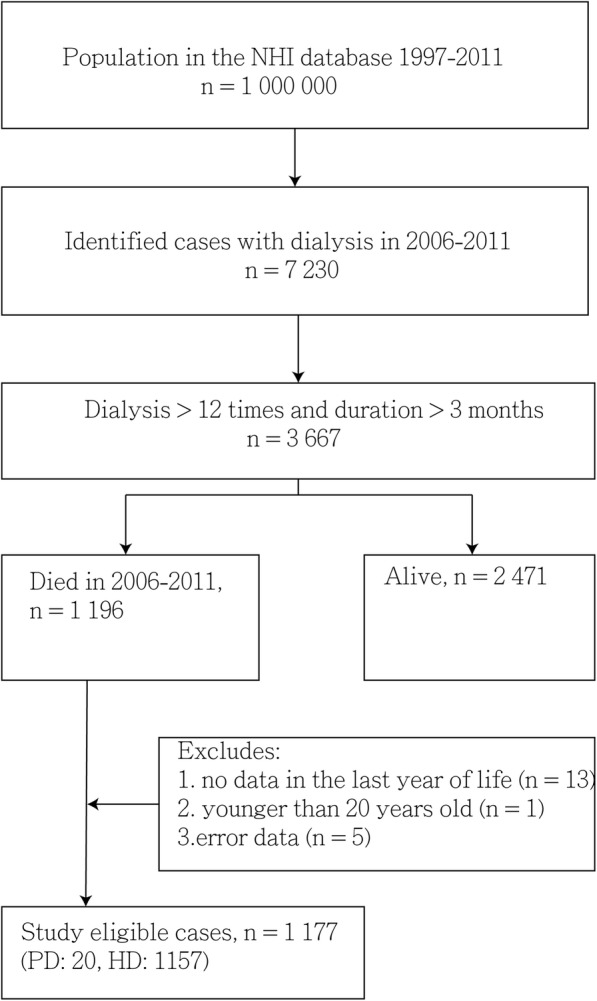
Methods: We conducted a population-based study and analyzed data from Taiwan's Longitudinal Health Insurance Database, which contains claims information of patient medical records, health care costs, and insurance system exit dates (our proxy for death between 2006 and 2011).
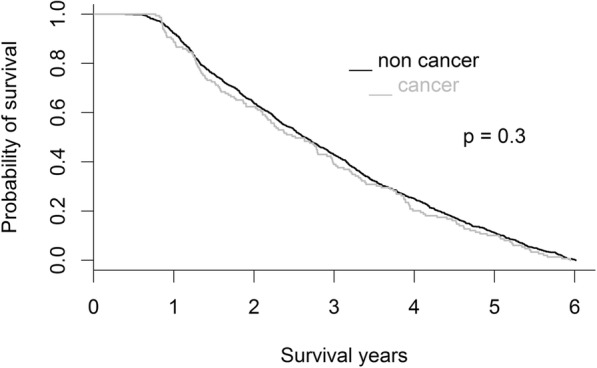
Results: Data of 1177 adult patients who died of chronic hemodialysis or peritoneal dialysis were investigated. The mean age of these patients was 69.7 ± 11.9 years, and 585 (49.7%) were women. Some patients with dialysis received cardiopulmonary resuscitation (66.9%), died in a hospital (65.0%), or were admitted to an intensive care unit (51.0%) in the last month of life. We further classified these patients into two groups, namely dialysis with cancer (DC) (n = 149) and dialysis without cancer (D) (n = 1028). Only 19 dialysis patients received palliative care, and the proportion of patients receiving palliative care was higher in the DC group than in the D group (11.4% vs. 0.2%). The mean health care costs per person during the final month of life was similar between the DC and D groups (USD 2755 ± 259 vs. USD 2827 ± 88). Multivariate logistic regression showed that the DC group had lower odds of receiving cardiopulmonary resuscitation (CPR) (OR: 0.39, CI = 0.26-0.56, p < 0.001) procedures, higher odds of longer hospital stays than the third quartile (> 25 days) (OR: 1.52, CI = 1.01-2.29, p = 0.0046), and higher odds of being hospitalized more than once (OR: 2.26, CI = 1.42-3.59, p = 0.001) than the D group in the last month of life after adjustments.
Conclusions: DC patients received hospice care more frequently, received CPR less frequently, and had similar health care costs. DC patients also had a higher risk of a hospital stay that lasted more than 25 days and more than one hospitalization compared with D patients in the final month of life.
Keywords: Cancer; Dialysis; End-of-life care.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- United States Renal Data System: Chapter 11: internal comparisons. Available from: https://www.usrds.org/2018/view/v2_11.aspx. Accessed 20 Oct 2018.
-
- Taiwan Society of Nephrology. Taiwan Renal Data System (TWRDS) 2014. 2014_ARKDT_table. Available from : http://www.tsn.org.tw/UI/H/H00201.aspx. Accessed 1 Jan 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
