

The impact of paid community health worker deployment on child survival: the connect randomized cluster trial in rural Tanzania
- PMID: 31311521
- PMCID: PMC6636132
- DOI: 10.1186/s12913-019-4203-1
The impact of paid community health worker deployment on child survival: the connect randomized cluster trial in rural Tanzania
Abstract
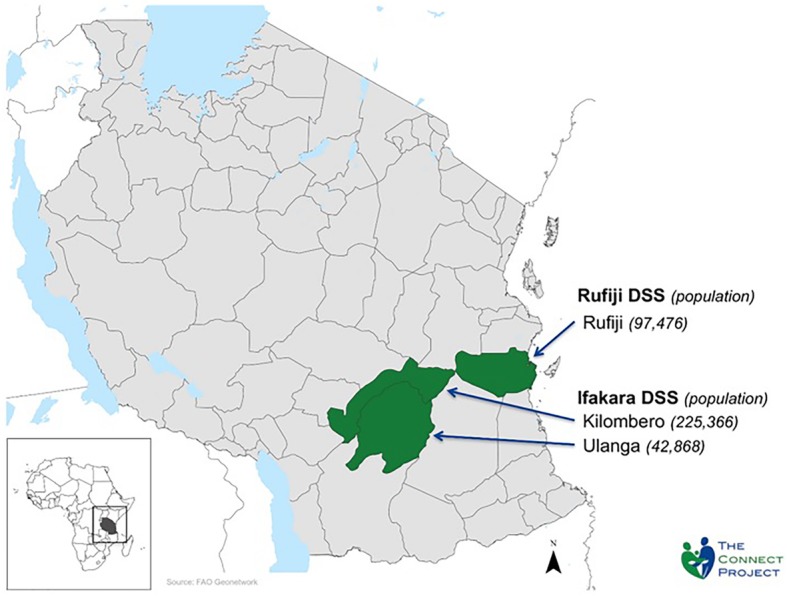
Background: This paper reports on a rigorously designed non-masked randomized cluster trial of the childhood survival impact of deploying paid community health workers to provide doorstep preventive, promotional, and curative antenatal, newborn, child, and reproductive health care in three rural Tanzanian districts.
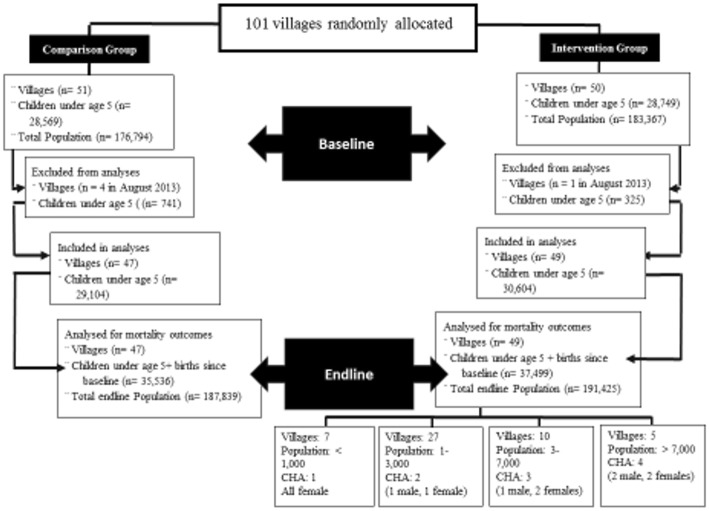
Methods: From August, 2011 to June 2015 ongoing demographic surveillance on 380,000 individuals permitted monitoring of neonatal, infant and under-5 mortality rates for 50 randomly selected intervention and 51 comparison villages. Over the initial 2 years of the project, logistics and supply support systems were managed by the Ifakara Health Institute. In 2013, the experiment transitioned its operational design to logistical support managed by the Ministry of Health and Social Welfare with the goal of enhancing government operational ownership and utilization of results for policy.
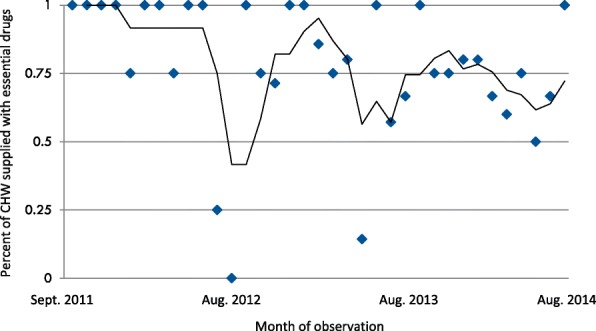
Results: The baseline under 5 mortality rate was 81.3 deaths per 1000 live births with a 95% confidence interval (CI) of 77.2-85.6 in the intervention group and 82.7/1000 (95% CI 78.5-87.1) in the comparison group yielding an adjusted hazard ratio (HR) of 0.99 (95% CI 0.88-1.11, p = 0.867). After 4 years of implementation, the under 5 mortality rate was 73.2/1000 (95% CI 69.3-77.3) in the intervention group and 77.4/1000 (95% CI 73.8-81.1) in the comparison group (adjusted HR 0.95 [95% CI 0.86-1.07], p = 0.443). The intervention had no impact on neonatal mortality in either the first 2 years (HR 1.10 [95% CI 0.89-1.36], p = .392) or last 2 years of implementation (HR 0.98 [95% CI 0.74-1.30], p = .902). Although community health worker deployment significantly reduced mortality among children aged 1-59 months during the first 2 years of implementation (HR 0.85 [95% CI 0.76-0.96], p = 0.008), mortality among post neonates was the same in both groups in years three and four (HR 1.03 [95% CI 0.85-1.24], p = 0.772). Results adjusted for stock-out effects show that diminishing impact was associated with logistics system lapses that constrained worker access to essential drugs and increased post-neonatal mortality risk in the final two project years (HR 1.42 [95% CI 1·07-1·88], p = 0·015).
Conclusions: Community health worker home-visit deployment had a null effect among neonates, and 2 years of initial impact among children over 1 month of age, but a null effect when tests were based on over 1 month of age data merged for all four project years. The atrophy of under age five effects arose because workers were not continuously equipped with essential medicines in years three and four. Analyses that controlled for stock-out effects suggest that adequately supplied workers had survival effects on children aged 1 to 59 months.
Trial registration: Registration for trial number ISRCTN96819844 was retrospectively completed on June 21, 2012.
Keywords: Childhood survival rate; Community health worker; Experimental trial; Health and Demographic Surveillance System; Implementation research; Integrated management of childhood illness; Primary health care; Randomized cluster trial; Tanzania; Under five mortality rate.
Conflict of interest statement
The Corresponding author is a member of the BMC Health Services Research Advisory Committee. Other authors of this publication have no competing interests to declare.
Figures
References
-
- United Nations The Millennium Development Goals Report 2012. New York: The United Nations; 2012. https://www.un.org/en/development/desa/publications/mdg-report-2012.html.
-
- Friberg Ingrid K., Kinney Mary V., Lawn Joy E., Kerber Kate J., Odubanjo M. Oladoyin, Bergh Anne-Marie, Walker Neff, Weissman Eva, Chopra Mickey, Black Robert E. Sub-Saharan Africa's Mothers, Newborns, and Children: How Many Lives Could Be Saved with Targeted Health Interventions? PLoS Medicine. 2010;7(6):e1000295. doi: 10.1371/journal.pmed.1000295. - DOI - PMC - PubMed
-
- Kassebaum NJ, Bertozzi-Villa A, Coggeshall MS, Shackelford KA, Steiner C, Heuton KR, et al. Global, regional, and national levels and causes of maternal mortality during 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet (London, England) 2014;384(9947):980–1004. doi: 10.1016/S0140-6736(14)60696-6. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
