

The association between pneumococcal vaccination, ethnicity, and the nasopharyngeal microbiota of children in Fiji
- PMID: 31311598
- PMCID: PMC6636143
- DOI: 10.1186/s40168-019-0716-4
The association between pneumococcal vaccination, ethnicity, and the nasopharyngeal microbiota of children in Fiji
Abstract
Background: Streptococcus pneumoniae is a significant global pathogen that colonises the nasopharynx of healthy children. Pneumococcal conjugate vaccines, which reduce nasopharyngeal colonisation of vaccine-type S. pneumoniae, may have broader effects on the nasopharyngeal microbiota; however, data are limited. In Fiji, nasopharyngeal carriage prevalence of S. pneumoniae and other colonising species differ between the two main ethnic groups. Here, we examined the association between the 7-valent pneumococcal conjugate vaccine (PCV7) and the nasopharyngeal microbiota of children in Fiji, including for each of the two main ethnic groups-indigenous Fijians (iTaukei) and Fijians of Indian descent (FID).
Method: The nasopharyngeal microbiota of 132 Fijian children was examined using nasopharyngeal swabs collected from 12-month-old iTaukei and FID children who were vaccinated (3 doses PCV7) or unvaccinated in infancy as part of a phase II randomised controlled trial. Microbiota composition was determined by sequencing the V4 region of the 16S rRNA gene. Species-specific carriage of S. pneumoniae, Haemophilus influenzae, Moraxella catarrhalis and Staphylococcus aureus was determined using real-time quantitative PCR. Associations between microbiota composition and other host and environmental factors were considered in the analysis.
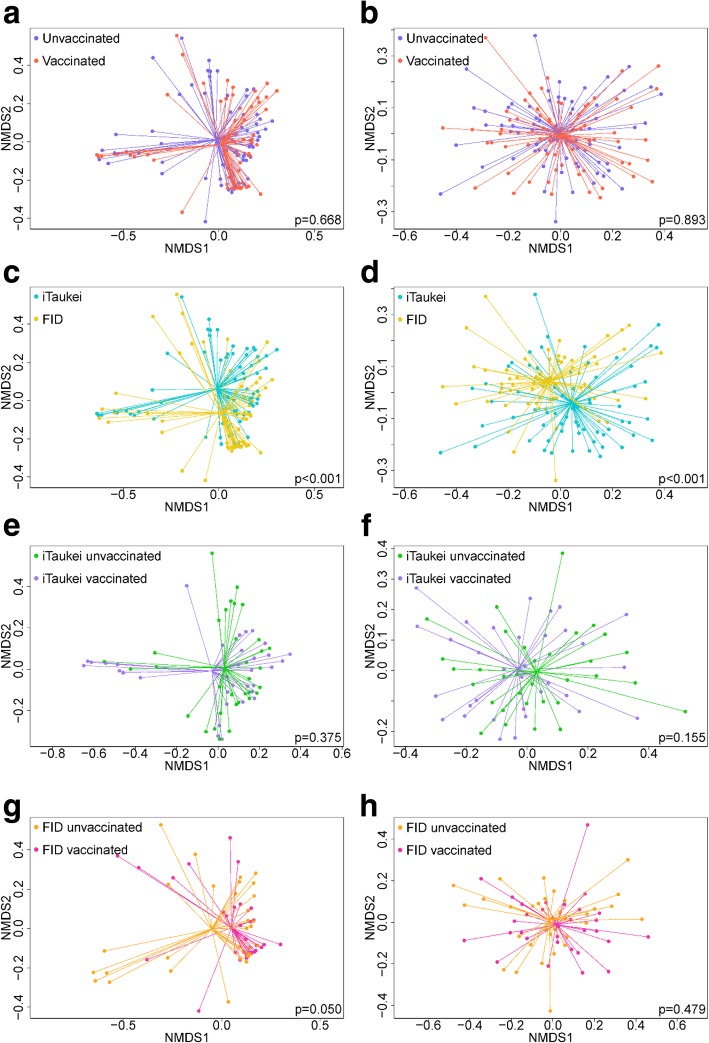
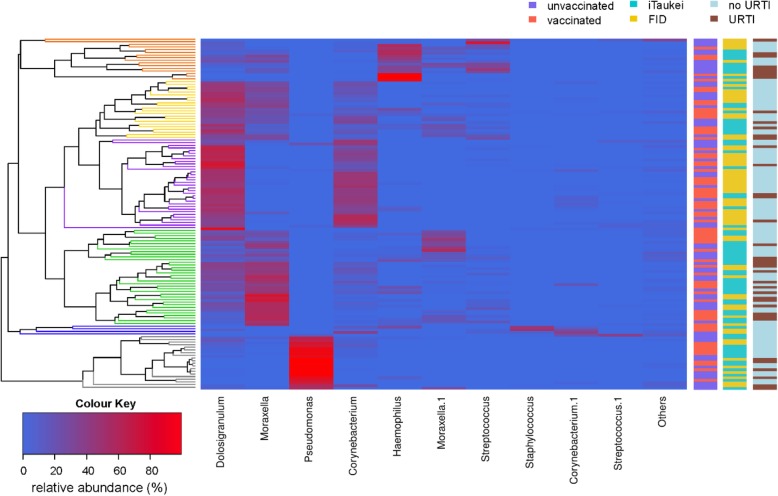
Results: PCV7 had no overall impact on microbial diversity or composition. However, ethnic differences were observed in both diversity and composition with iTaukei children having higher relative abundance of Moraxella (p = 0.004) and Haemophilus (p = 0.004) and lower relative abundance of Staphylococcus (p = 0.026), Dolosigranulum (p = 0.004) and Corynebacterium (p = 0.003) compared with FID children. Further, when we stratified by ethnicity, associations with PCV7 could be detected: vaccinated iTaukei children had a lower relative abundance of Streptococcus and Haemophilus compared with unvaccinated iTaukei children (p = 0.022 and p = 0.043, respectively); and vaccinated FID children had a higher relative abundance of Dolosigranulum compared with unvaccinated FID children (p = 0.037). Children with symptoms of an upper respiratory tract infection (URTI) had a significantly different microbiota composition to children without symptoms. The microbiota composition of iTaukei children without URTI symptoms was most similar to the microbiota composition of FID children with URTI symptoms.
Conclusions: Associations between PCV7 and nasopharyngeal microbiota differed within each ethnic group. This study highlights the influence that ethnicity and URTIs have on nasopharyngeal microbiota.
Keywords: Ethnicity; Fiji; Nasopharyngeal microbiota; Pneumococcal conjugate vaccination; Streptococcus pneumoniae.
Conflict of interest statement
CS, EMD, CDN and EKM are investigators on a clinical research collaboration with Pfizer investigating the impact of PCV on adult pneumonia in Mongolia. MH received consultancy fees and has been awarded investigator initiated research grants from Pfizer, not related to this work. The other authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
