

IgA Nephropathy in Elderly Patients
- PMID: 31311818
- PMCID: PMC6682823
- DOI: 10.2215/CJN.13251118
IgA Nephropathy in Elderly Patients
Abstract
Background and objectives: Some studies suggest that the incidence of IgA nephropathy is increasing in older adults, but there is a lack of information about the epidemiology and behavior of the disease in that age group.
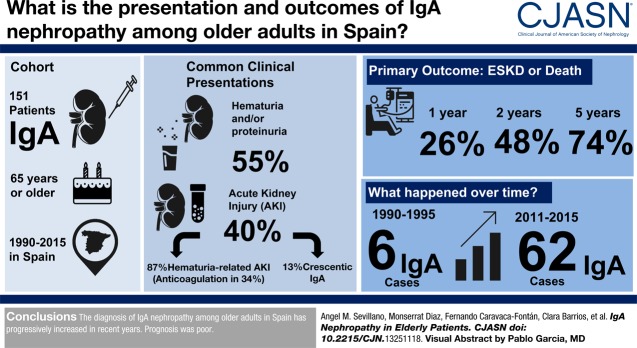
Design, setting, participants, & measurements: In this retrospective multicentric study, we analyzed the incidence, forms of presentation, clinical and histologic characteristics, treatments received, and outcomes in a cohort of 151 patients ≥65 years old with biopsy-proven IgA nephropathy diagnosed between 1990 and 2015. The main outcome was a composite end point of kidney replacement therapy or death before kidney replacement therapy.
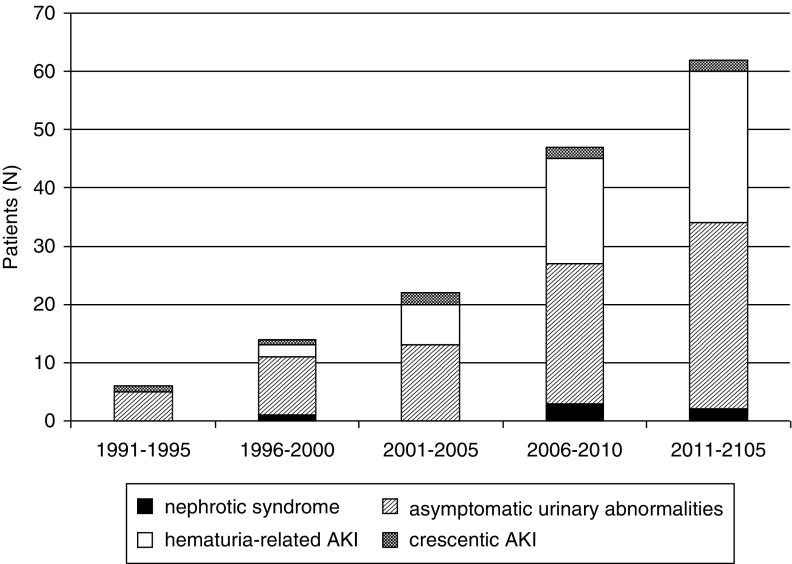
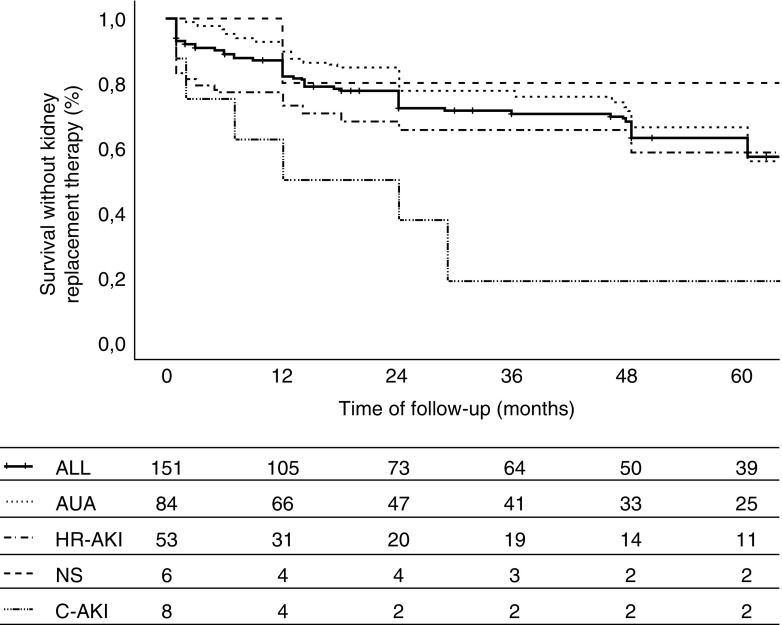
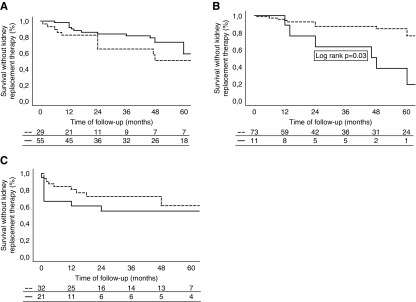
Results: We found a significant increase in the diagnosis of IgA nephropathy over time from six patients in 1990-1995 to 62 in 2011-2015 (P value for trend =0.03). After asymptomatic urinary abnormalities (84 patients; 55%), AKI was the most common form of presentation (61 patients; 40%). Within the latter, 53 (86%) patients presented with hematuria-related AKI (gross hematuria and tubular necrosis associated with erythrocyte casts as the most important lesions in kidney biopsy), and eight patients presented with crescentic IgA nephropathy. Six (4%) patients presented with nephrotic syndrome. Among hematuria-related AKI, 18 (34%) patients were receiving oral anticoagulants, and this proportion rose to 42% among the 34 patients older than 72 years old who presented with hematuria-related AKI. For the whole cohort, survival rates without the composite end point were 74%, 48%, and 26% at 1, 2, and 5 years, respectively. Age, serum creatinine at presentation, and the degree of interstitial fibrosis in kidney biopsy were risk factors significantly associated with the outcome, whereas treatment with renin-angiotensin-aldosterone blockers was associated with a lower risk. Immunosuppressive treatments were not significantly associated with the outcome.
Conclusions: The diagnosis of IgA nephropathy among older adults in Spain has progressively increased in recent years, and anticoagulant therapy may be partially responsible for this trend. Prognosis was poor.
Podcast: This article contains a podcast at https://www.asn-online.org/media/podcast/CJASN/2019_07_16_CJASNPodcast_19_08_.mp3.
Keywords: Angiotensins; Anticoagulants; Biopsy; Erythrocytes; Glomerulonephritis, IGA; Hematuria; IgA nephropathy; Incidence; Kidney Function Tests; Prognosis; Renal Replacement Therapy; Renin; Retrospective Studies; acute kidney injury; acute renal failure; aldosterone; anticoagulation therapy; creatinine; hematuria; nephrotic syndrome; risk factors.
Copyright © 2019 by the American Society of Nephrology.
Figures
References
-
- Floege J, Feehally J: Treatment of IgA nephropathy and Henoch-Schönlein nephritis. Nat Rev Nephrol 9: 320–327, 2013 - PubMed
-
- Lai KN, Tang SCW, Schena FP, Novak J, Tomino Y, Fogo AB, Glassock RJ: IgA nephropathy. Nat Rev Dis Primers 2: 16001, 2016 - PubMed
-
- Gutiérrez E, Praga M, Rivera F, Sevillano A, Yuste C, Goicoechea M, López-Gómez JM; all members of the Spanish Registry of Glomerulonephritis : Changes in the clinical presentation of immunoglobulin A nephropathy: Data from the Spanish registry of glomerulonephritis. Nephrol Dial Transplant 33: 472–477, 2018 - PubMed
-
- Duan ZY, Cai GY, Chen YZ, Liang S, Liu SW, Wu J, Qiu Q, Lin SP, Zhang XG, Chen XM: Aging promotes progression of IgA nephropathy: A systematic review and meta-analysis. Am J Nephrol 38: 241–252, 2013 - PubMed
