

Challenging clubfeet: the arthrogrypotic clubfoot and the complex clubfoot
- PMID: 31312267
- PMCID: PMC6598040
- DOI: 10.1302/1863-2548.13.190072
Challenging clubfeet: the arthrogrypotic clubfoot and the complex clubfoot
Abstract
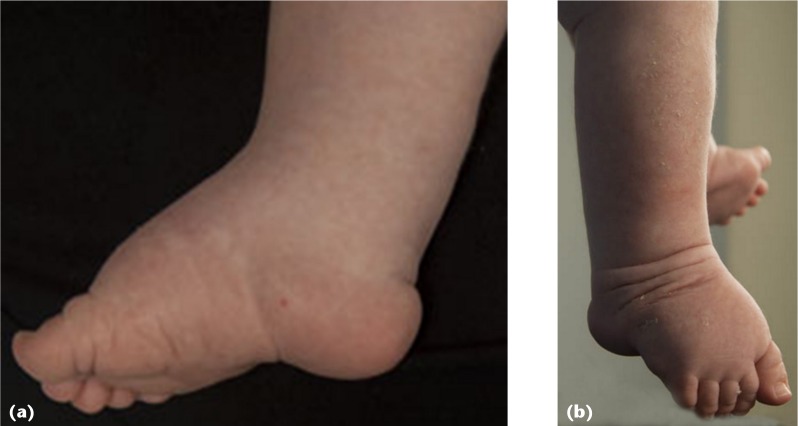
Within the realm of clubfoot deformities, teratologic and complex (or atypical) clubfeet stand out as the most difficult. Exemplarities of the teratologic types of clubfoot are those associated with arthrogryposis multiplex congenita. Treatment of arthrogrypotic clubfoot deformities has been controversial; many different procedures have been advocated, with variable success rates. These clubfeet have a high recurrence rate, regardless of treatment type. Often, the high recurrence rate has led to a high repeat surgery rate, and poor outcomes. Treatment strategies should highlight care that avoids the development of a stiffened foot and allows for a variety of options to regain correction when a relapse occurs. Modifications of the Ponseti method for idiopathic clubfeet have been successful in managing the deformity. The equinocavus variant of the arthrogrypotic clubfoot should be distinguished from the classic clubfoot, as it requires a different treatment method. The equinocavus clubfoot is very similar to the complex or atypical clubfoot. The complex, or atypical, clubfoot also requires a different treatment strategy compared with the typical idiopathic congenital clubfoot. The complex clubfoot appears to be idiopathic in some cases and iatrogenic (due to slipping stretching casts) in others. Dr. Ponseti's modification of his protocol has been effective in treating the deformity. The high recurrence rate suggests the difficulty in maintaining the deformity after correction. The author's preferred treatment for each deformity is included, with an emphasis on minimally invasive methods.
Level of evidence: Level V, expert opinion.
Keywords: Ponseti; arthrogryposis; arthrogryposis multiplex congenita; arthrogrypotic clubfoot; atypical clubfoot; clubfeet; complex clubfoot.
Figures






References
-
- Ponseti IV, Smoley EN. Congenital club foot: The results of treatment. J Bone Joint Surg [Am] 1963;45-A:261–275.
-
- Ponseti IV. Congenital clubfoot: fundamentals of treatment. New York, NY: Oxford University Press Inc, 1996.
-
- Ponseti IV, Zhivkov M, Davis N, et al. . Treatment of the complex idiopathic clubfoot. Clin Orthop Relat Res 2006;451:171–176. - PubMed
-
- Hall JG. Arthrogryposis multiplex congenita: etiology, genetics, classification, diagnostic approach, and general aspects. J Pediatr Orthop B 1997;6:159–166. - PubMed
-
- Bevan WP, Hall JG, Bamshad M, et al. . Arthrogryposis multiplex congenita (amyoplasia): an orthopaedic perspective. J Pediatr Orthop 2007;27:594–600. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
