

Treatment of relapsed, residual and neglected clubfoot: adjunctive surgery
- PMID: 31312269
- PMCID: PMC6598039
- DOI: 10.1302/1863-2548.13.190079
Treatment of relapsed, residual and neglected clubfoot: adjunctive surgery
Abstract
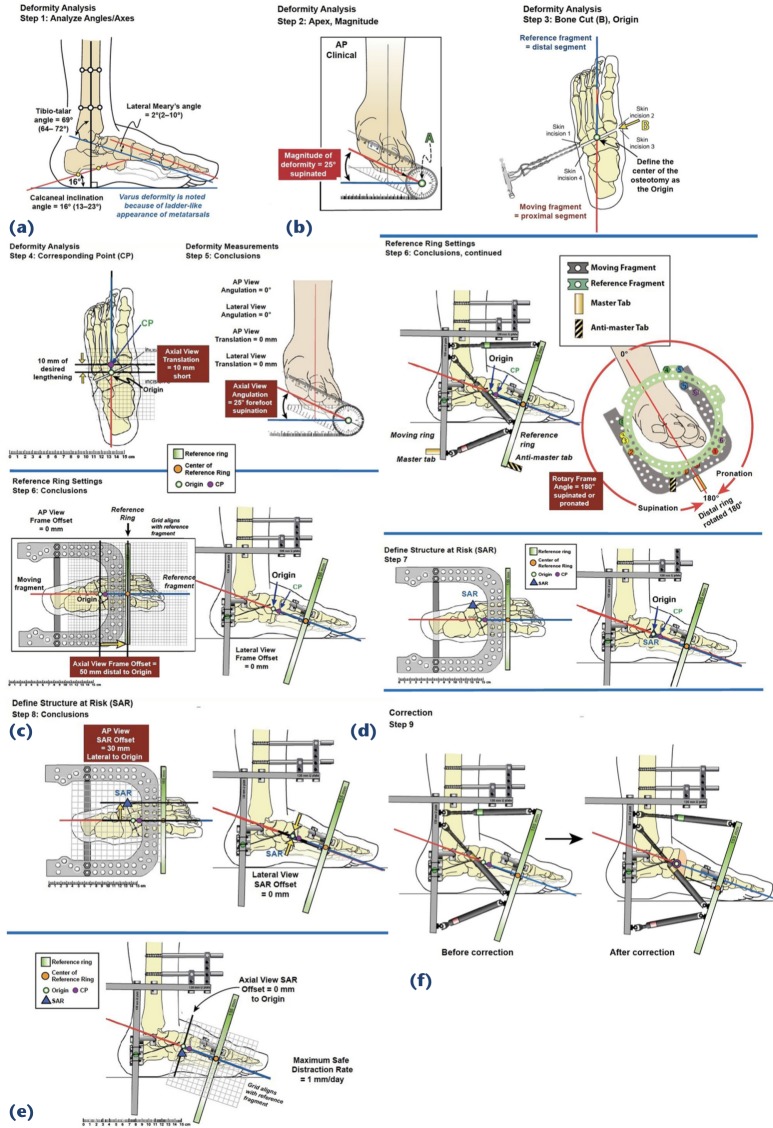
Over the past two decades, the Ponseti 'conservative' (non-surgical) method of clubfoot treatment has been almost universally adopted worldwide. As a result, the need for operative treatment for clubfoot has decreased dramatically. However, even Ponseti himself routinely used surgery for certain patients: at least 90% of feet need percutaneous tenotomy, and 15% to 40% may require tibialis anterior tendon transfer. Additionally, relapses are common, sometimes necessitating further surgical intervention. Relapses are recurrent deformities in previously well corrected feet. Residual deformities may be defined as persistent deformities in incompletely corrected feet. In addition, in many parts of the developing world, neglected clubfoot is still a major challenge. Many neglected feet can be treated with Ponseti principles, particularly in younger children. However, in older children and adults, surgical approaches are more likely to be needed. Major reasons for relapsed/residual clubfoot include incomplete application of the Ponseti principles, inability to adhere to the foot abduction brace protocol, failure to recommend a complete course of bracing and inadequate follow-up. Sometimes, despite excellent treatment, and perfect adherence to the bracing protocols, there are still relapses, related to intrinsic muscle imbalance. We describe several solutions that include reinstitution of Ponseti casting and 'á la carte' operative treatment. As an alternative for particularly stubborn cases, application of a hexapod external fixator can be a powerful tool. In order to be a full-service clubfoot specialist, and not only a Ponseti practitioner, one must have in their toolbox the full gamut of adjunctive surgical options.
Level of evidence: V.
Keywords: clubfoot; neglected; relapsed; residual.
Figures





References
-
- Wenger DR, Rang M The art and practice of children orthopedics. New York: Raven Press, 1992.
-
- Ponseti IV, Smoley EN. Congenital club foot: the results of treatment. J Bone Joint Surg [Am] 1963;45-A:261-344.
-
- Ponseti IV. Congenital clubfoot: fundamentals of treatment. New York: Oxford University Inc, 1996.
-
- Coplan JA, Herzenberg JE. Non-operative treatment of congenital clubfoot : McCarthy JJ, Drennan JC The child’s foot and ankle (2nd edition). Philadelphia: Lippincott Williams &Wilkins, 2010:64-74.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
