

Glans Resurfacing with Skin Graft for Penile Cancer: A Step-by-Step Video Presentation of the Technique and Review of the Literature
- PMID: 31312658
- PMCID: PMC6595175
- DOI: 10.1155/2019/5219048
Glans Resurfacing with Skin Graft for Penile Cancer: A Step-by-Step Video Presentation of the Technique and Review of the Literature
Abstract
Introduction: Glans resurfacing has been suggested as a treatment option for the surgical management of superficial penile cancer (Tis, Ta, T1aG1, T1aG2). In this article we describe in detail the glans resurfacing technique with skin graft for penile cancer in a video presentation and we review the current knowledge of the literature.
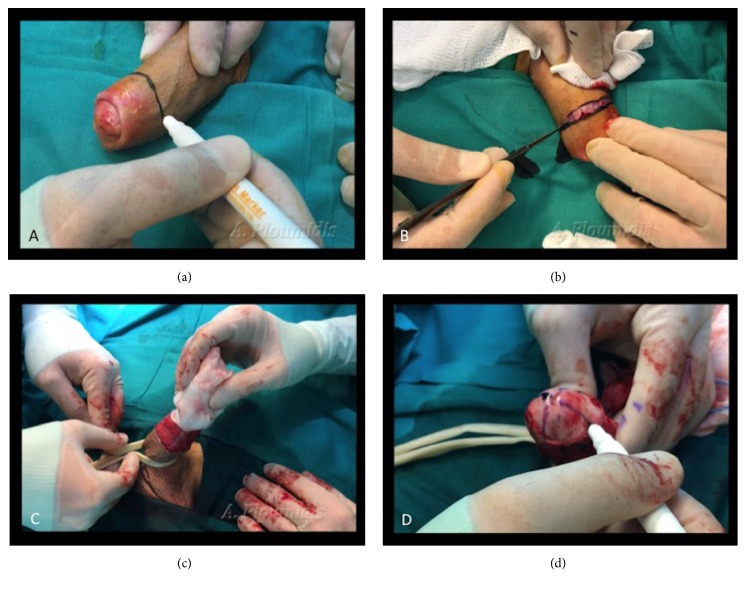
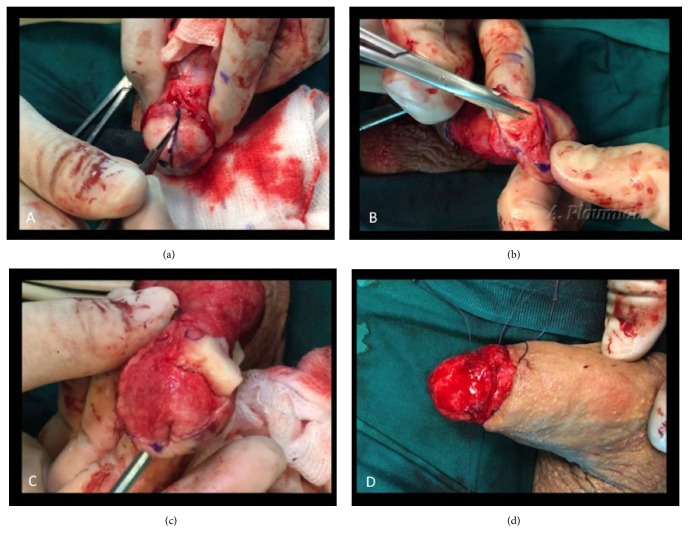
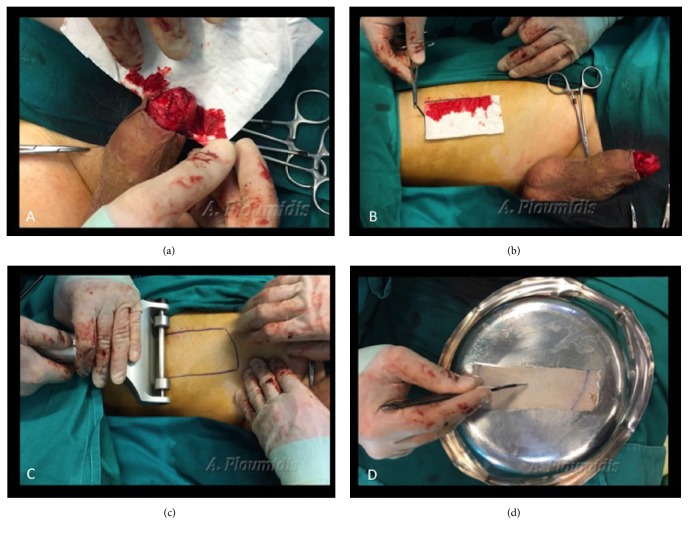
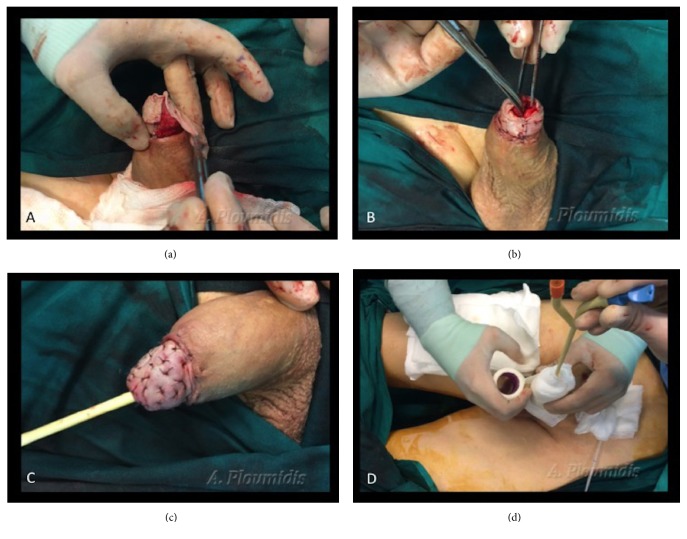
Material and methods: The procedure is described in a stepwise fashion. Initially the patient is circumcised. The glans is marked in quadrants and completely stripped by dissecting and removing the epithelium and subepithelium layer of the glans. Deep spongiosal biopsies are taken to exclude invasion. Each quadrant is sent separately for biopsy. The surface of the graft size needed is estimated. A partial thickness skin graft is harvested from the thigh with a dermatome. The skin graft is then fenestrated. The graft is rolled over the glans and quilted with multiple sutures. A silicone 16F Foley catheter and a suprapubic catheter are placed. The penis is dressed with multiple gauzes and compressed with an elastic band.
Results: The patient is discharged the next day. The dressing and Foley catheter are removed in 7 days. The patient continues to use the suprapubic catheter for 7 more days. The patient refrains from any sexual activity for 6 weeks and is closely followed.
Conclusions: Glans resurfacing is an emerging new appealing surgical technique that is already a recommendation in the EAU guidelines for the treatment of premalignant and superficial penile lesions. The overall satisfaction rate and recovery of the sexual function are acceptable, and it can be considered an ideal procedure to treat superficial penile cancer.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
