

Breastfeeding, Cellular Immune Activation, and Myocardial Recovery in Peripartum Cardiomyopathy
- PMID: 31312753
- PMCID: PMC6609998
- DOI: 10.1016/j.jacbts.2019.01.010
Breastfeeding, Cellular Immune Activation, and Myocardial Recovery in Peripartum Cardiomyopathy
Abstract
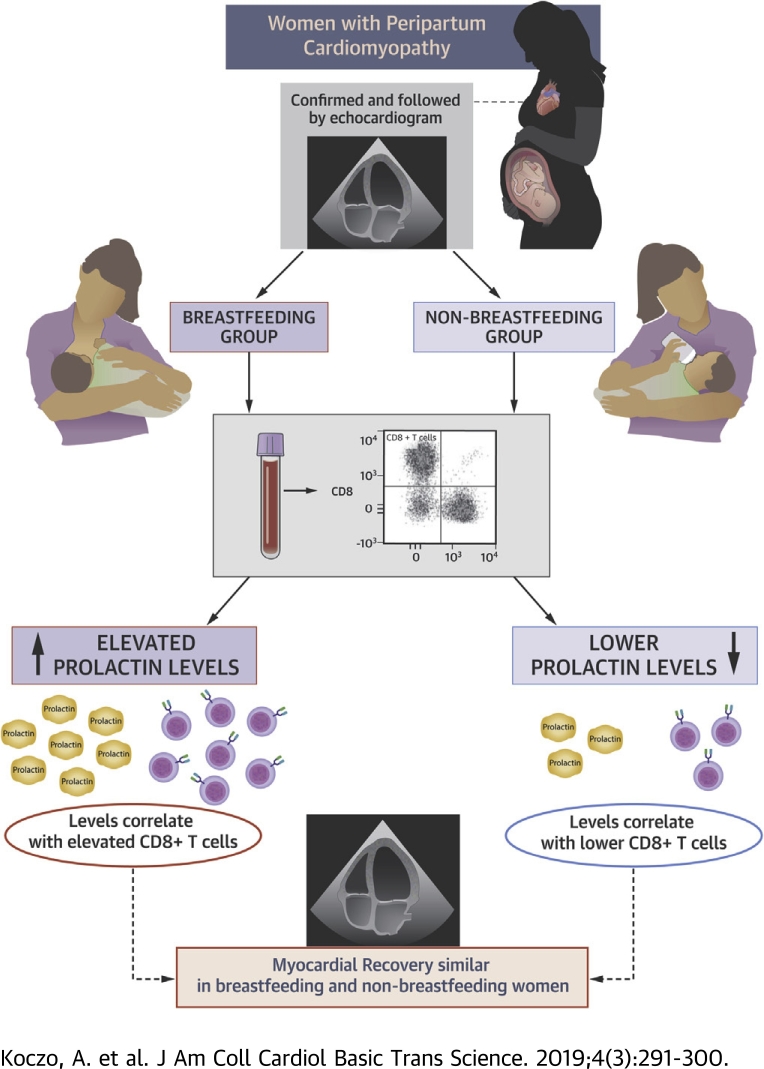
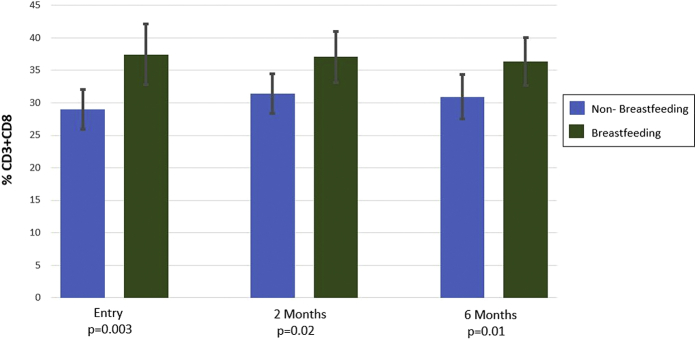
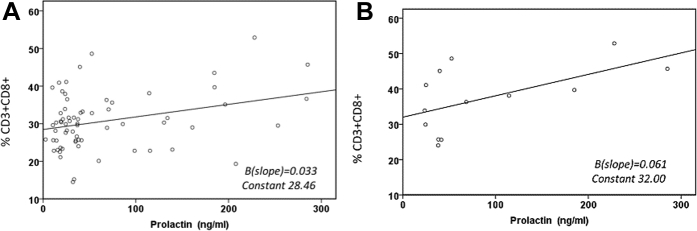
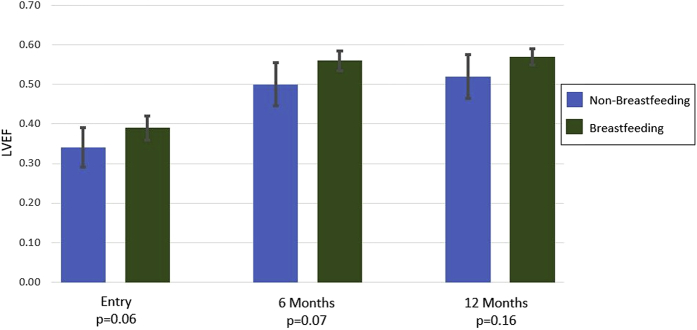
The etiology of peripartum cardiomyopathy remains unknown. One hypothesis is that an increase in the 16-kDa form of prolactin is pathogenic and suggests that breastfeeding may worsen peripartum cardiomyopathy by increasing prolactin, while bromocriptine, which blocks prolactin release, may be therapeutic. An autoimmune etiology has also been proposed. The authors investigated the impact of breastfeeding on cellular immunity and myocardial recovery for women with peripartum cardiomyopathy in the IPAC (Investigations in Pregnancy Associated Cardiomyopathy) study. Women who breastfed had elevated prolactin, and prolactin levels correlated with elevations in CD8+ T cells. However, despite elevated prolactin and cytotoxic T cell subsets, myocardial recovery was not impaired in breastfeeding women.
Keywords: BF, breastfeeding; LVEF, left ventricular ejection fraction; NBF, nonbreastfeeding; PPCM, peripartum cardiomyopathy; breastfeeding; immune activation; peripartum cardiomyopathy.
Figures
References
-
- Hilfiker-Kleiner D., Sliwa K. Pathophysiology and epidemiology of peripartum cardiomyopathy. Nat Rev Cardiol. 2014;11:364–370. - PubMed
-
- Arany Z., Elkayam U. Peripartum cardiomyopathy. Circulation. 2016;133:1397–1409. - PubMed
-
- Ansari A., Fett J.D., Carraway R.E. Autoimmune mechanisms as the basis for human peripartum cardiomyopathy. Clin Rev Allergy Immunol. 2002;23:301–324. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
