

WHIM Syndrome: from Pathogenesis Towards Personalized Medicine and Cure
- PMID: 31313072
- PMCID: PMC6698215
- DOI: 10.1007/s10875-019-00665-w
WHIM Syndrome: from Pathogenesis Towards Personalized Medicine and Cure
Abstract
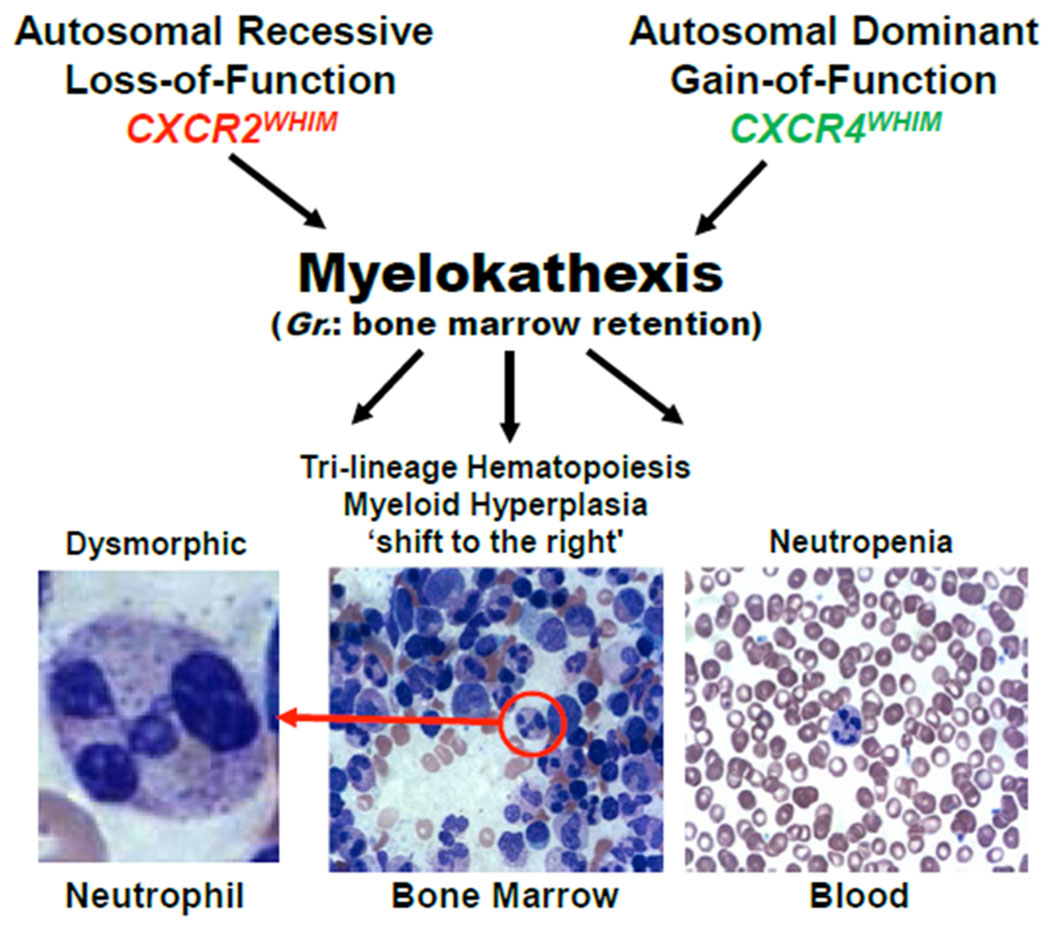
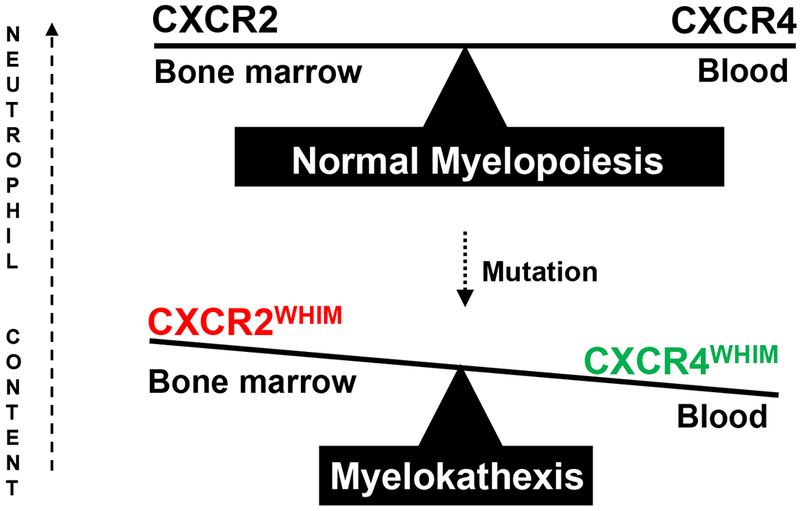
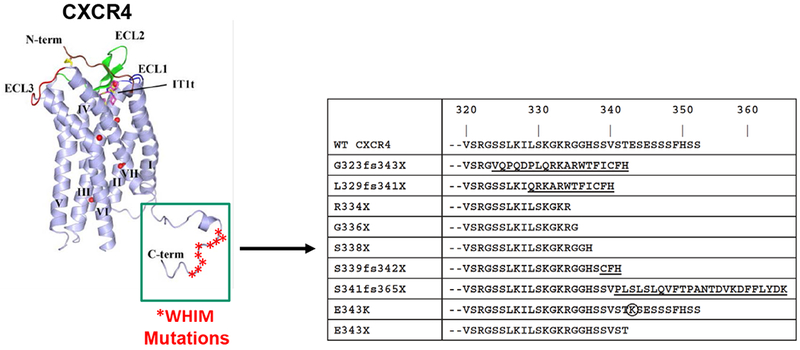
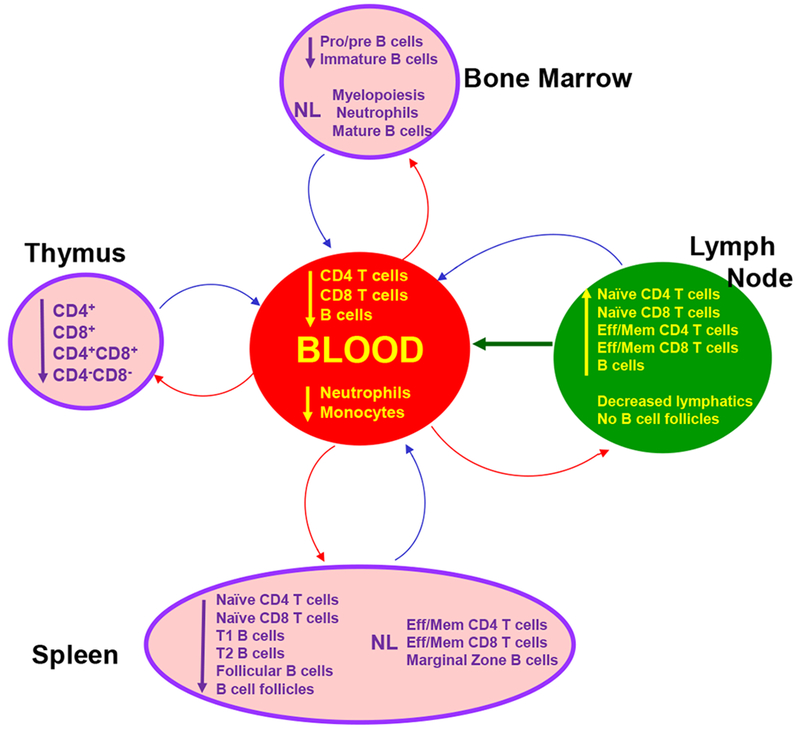
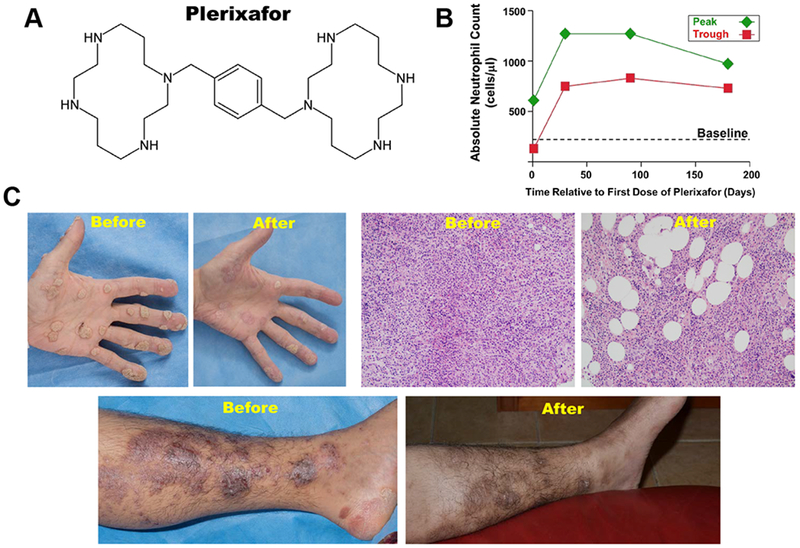
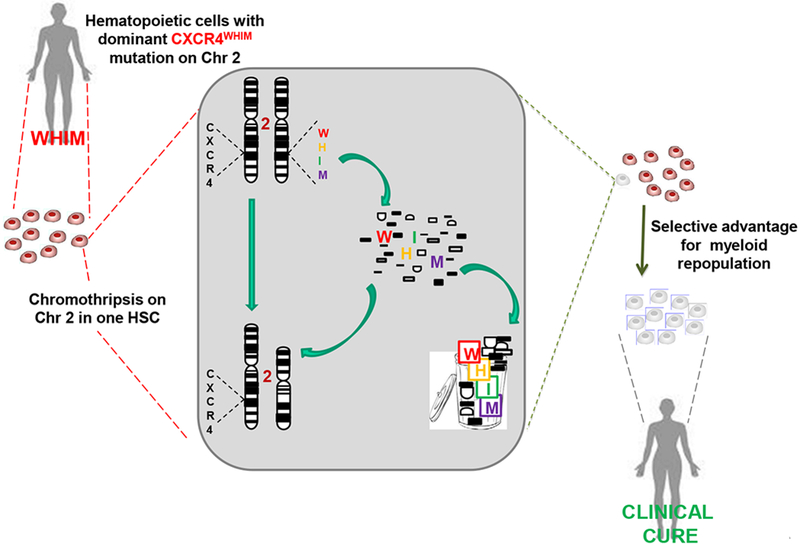
WHIM syndrome is a rare combined primary immunodeficiency disease named by acronym for the diagnostic tetrad of warts, hypogammaglobulinemia, infections, and myelokathexis. Myelokathexis is a unique form of non-cyclic severe congenital neutropenia caused by accumulation of mature and degenerating neutrophils in the bone marrow; monocytopenia and lymphopenia, especially B lymphopenia, also commonly occur. WHIM syndrome is usually caused by autosomal dominant mutations in the G protein-coupled chemokine receptor CXCR4 that impair desensitization, resulting in enhanced and prolonged G protein- and β-arrestin-dependent responses. Accordingly, CXCR4 antagonists have shown promise as mechanism-based treatments in phase 1 clinical trials. This review is based on analysis of all 105 published cases of WHIM syndrome and covers current concepts, recent advances, unresolved enigmas and controversies, and promising future research directions.
Keywords: CXCL12; CXCR2; CXCR4; Chemokine; human papillomavirus; myelokathexis; plerixafor.
Conflict of interest statement
Conflict of Interest Statement
PMM is a member of the Scientific Advisory Board of X4-Pharma. PMM, J-LG and DHM are listed as inventors on a patent application disclosing a method of enhancing hematopoietic stem cell engraftment by CXCR4 knockdown. There are no other stated conflicts of interest.
Figures
References
-
- Krill CE, Smith HD, Mauer AM. Chronic Idiopathic Granulocytopenia. New England Journal of Medicine. 1964;270:973–9. - PubMed
-
- Zuelzer WW. “MYELOKATHEXIS”--A NEW FORM OF CHRONIC GRANULOCYTOPENIA. REPORT OF A CASE. N Engl J Med 1964;270:699–704. - PubMed
-
- O’Regan S, Newman AJ, Graham RC. “Myelokathexis”. Neutropenia with marrow hyperplasia. Am J Dis Child. 1977;131:655–8. - PubMed
-
- Mentzer WC, Johnston RB, Baehner RL, Nathan DG. An unusual form of chronic neutropenia in a father and daughter with hypogammaglobulinaemia. Br J Haematol 1977;36:313–22. - PubMed
-
- Bohinjec J Myelokathexis: chronic neutropenia with hyperplastic bone marrow and hypersegmented neutrophils in two siblings. Blut. 1981;42:191–6. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
