

Effect of Simvastatin-Ezetimibe Compared With Simvastatin Monotherapy After Acute Coronary Syndrome Among Patients 75 Years or Older: A Secondary Analysis of a Randomized Clinical Trial
- PMID: 31314050
- PMCID: PMC6647004
- DOI: 10.1001/jamacardio.2019.2306
Effect of Simvastatin-Ezetimibe Compared With Simvastatin Monotherapy After Acute Coronary Syndrome Among Patients 75 Years or Older: A Secondary Analysis of a Randomized Clinical Trial
Abstract
Importance: Limited evidence is available regarding the benefit and hazard of higher-intensity treatment to lower lipid levels among patients 75 years or older. As a result, guideline recommendations differ for this age group compared with younger patients.
Objective: To determine the effect on outcomes and risks of combination ezetimibe and simvastatin compared with simvastatin monotherapy to lower lipid levels among patients 75 years or older with stabilized acute coronary syndrome (ACS).
Design, setting, participants: In this prespecified secondary analysis of the global, multicenter, prospective clinical randomized Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT), outcomes and risks were compared by age among patients 50 years or older after a hospitalization for ACS. Data were collected from October 26, 2005, through July 8, 2010, with the database locked October 21, 2014. Data were analyzed May 29, 2015, through March 13, 2018, using Kaplan-Meier curves and Cox proportional hazards models.
Interventions: Double-blind randomized assignment to combined simvastatin and ezetimibe or simvastatin and placebo with follow-up for a median of 6 years (interquartile range, 4.3-7.1 years).
Main outcomes and measures: The primary composite end point consisted of death due to cardiovascular disease, myocardial infarction (MI), stroke, unstable angina requiring hospitalization, and coronary revascularization after 30 days. Individual adverse ischemic and safety end points and lipid variables were also analyzed.
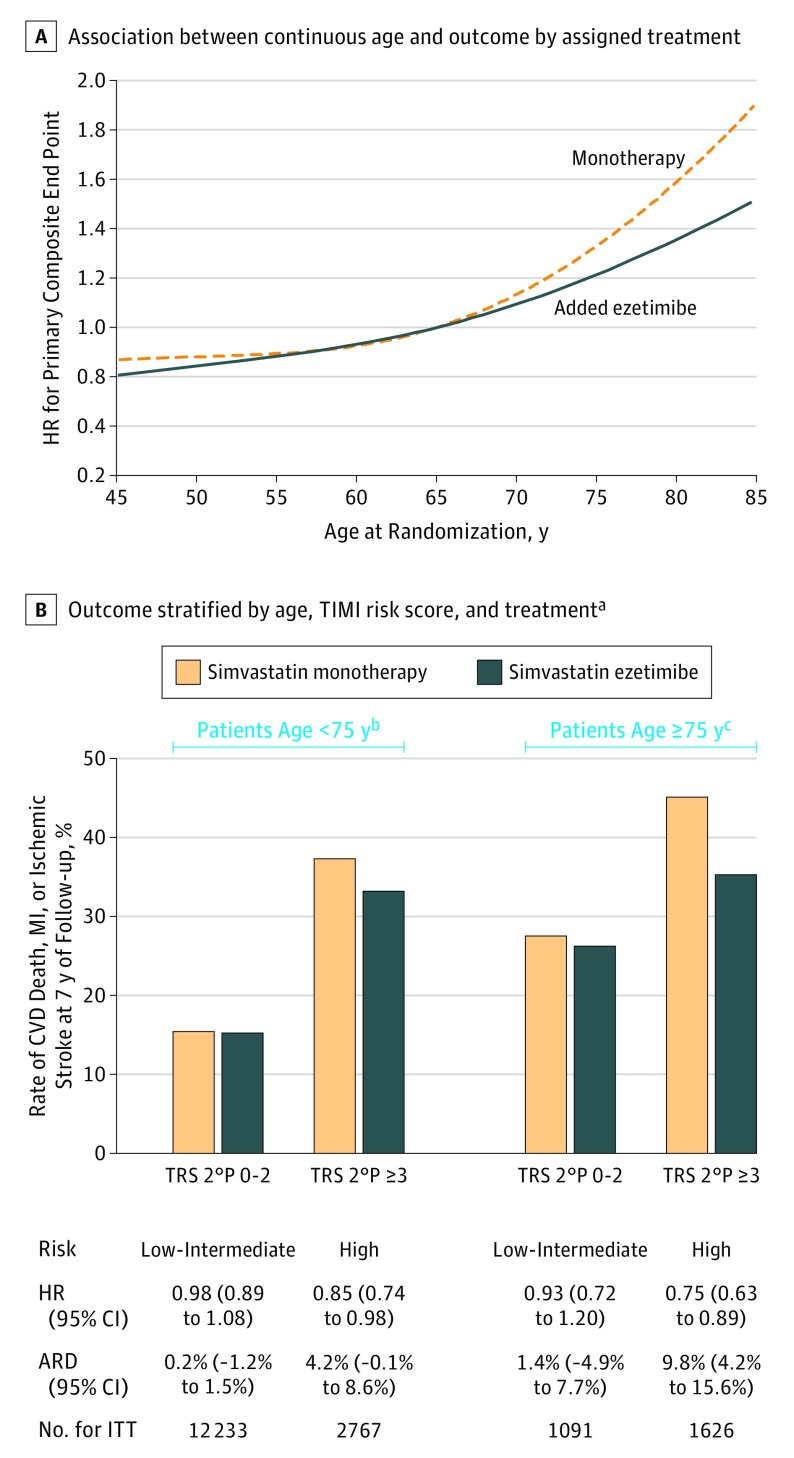
Results: Of 18 144 patients enrolled (13 728 men [75.7%]; mean [SD] age, 64.1 [9.8] years), 5173 (28.5%) were 65 to 74 years old, and 2798 (15.4%) were 75 years or older at randomization. Treatment with simvastatin-ezetimibe resulted in lower rates of the primary end point than simvastatin-placebo, including 0.9% for patients younger than 65 years (HR, 0.97; 95% CI, 0.90-1.05) and 0.8% for patients 65 to 74 years of age (hazard ratio [HR], 0.96; 95% CI, 0.87-1.06), with the greatest absolute risk reduction of 8.7% for patients 75 years or older (HR, 0.80; 95% CI, 0.70-0.90) (P = .02 for interaction). The rate of adverse events did not increase with simvastatin-ezetimibe vs simvastatin-placebo among younger or older patients.
Conclusions and relevance: In IMPROVE-IT, patients hospitalized for ACS derived benefit from higher-intensity therapy to lower lipid levels with simvastatin-ezetimibe compared with simvastatin monotherapy, with the greatest absolute risk reduction among patients 75 years or older. Addition of ezetimibe to simvastatin was not associated with any significant increase in safety issues among older patients. These results may have implications for guideline recommendations regarding lowering of lipid levels in the elderly.
Trial registration: ClinicalTrials.gov identifier: NCT00202878.
Conflict of interest statement
Figures


Comment in
-
Intensive Lipid Lowering in Elderly Patients.JAMA Cardiol. 2019 Sep 1;4(9):855-856. doi: 10.1001/jamacardio.2019.2333. JAMA Cardiol. 2019. PMID: 31314042 No abstract available.
-
Interpreting the Benefit of Simvastatin-Ezetimibe in Patients 75 Years or Older.JAMA Cardiol. 2020 Feb 1;5(2):235. doi: 10.1001/jamacardio.2019.5200. JAMA Cardiol. 2020. PMID: 31895431 Free PMC article. No abstract available.
-
Interpreting the Benefit of Simvastatin-Ezetimibe in Patients 75 Years or Older-Reply.JAMA Cardiol. 2020 Feb 1;5(2):235-236. doi: 10.1001/jamacardio.2019.5241. JAMA Cardiol. 2020. PMID: 31895449 No abstract available.
-
Interpreting the Benefit of Simvastatin-Ezetimibe in Patients 75 Years or Older.JAMA Cardiol. 2020 Feb 1;5(2):234. doi: 10.1001/jamacardio.2019.5197. JAMA Cardiol. 2020. PMID: 31895451 No abstract available.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. ; Writing Group Members; American Heart Association Statistics Committee; Stroke Statistics Subcommittee . Heart disease and stroke statistics-2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38-e360. - PubMed
-
- Colby SL, Ortman JM. The Baby Boom Cohort in the United States: 2012 to 2060. Current Population Reports, P25-1141. Washington, DC: US Census Bureau; May 2014. available at https://www.census.gov/content/dam/Census/library/publications/2014/demo.... Accessed October 11, 2016.
-
- Fulcher J, O’Connell R, Voysey M, et al. ; Cholesterol Treatment Trialists’ (CTT) Collaboration . Efficacy and safety of LDL-lowering therapy among men and women: meta-analysis of individual data from 174,000 participants in 27 randomised trials. Lancet. 2015;385(9976):1397-1405. doi:10.1016/S0140-6736(14)61368-4 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
