

Urine Tenofovir Concentrations Correlate With Plasma and Relate to Tenofovir Disoproxil Fumarate Adherence: A Randomized, Directly Observed Pharmacokinetic Trial (TARGET Study)
- PMID: 31314073
- PMCID: PMC7201421
- DOI: 10.1093/cid/ciz645
Urine Tenofovir Concentrations Correlate With Plasma and Relate to Tenofovir Disoproxil Fumarate Adherence: A Randomized, Directly Observed Pharmacokinetic Trial (TARGET Study)
Erratum in
-
Erratum.Clin Infect Dis. 2019 Oct 15;69(9):1647. doi: 10.1093/cid/ciz798. Clin Infect Dis. 2019. PMID: 31600383 Free PMC article. No abstract available.
Abstract
Background: Direct measurement of tenofovir (TFV) in urine could be an objective measure to monitor adherence to preexposure prophylaxis (PrEP) or TFV-based antiretroviral therapy (ART).
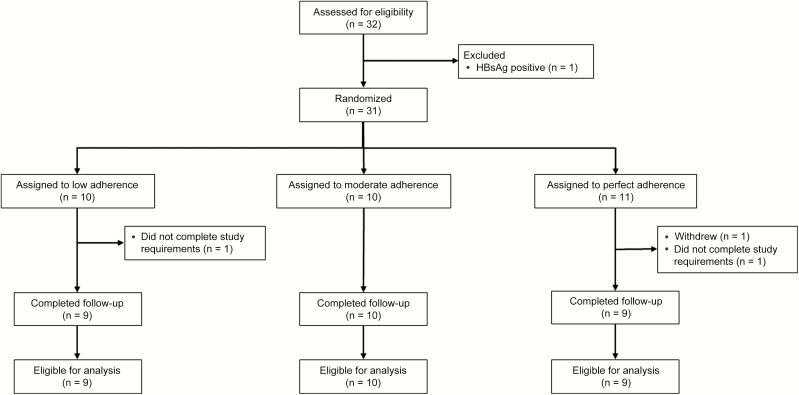
Methods: We conducted a 3-arm randomized, pharmacokinetic study of tenofovir disoproxil fumarate (TDF) 300 mg/emtricitabine (FTC) 200 mg among adults living with human immunodeficiency virus. Participants were randomized to receive controlled TDF/FTC dosing as (1) "perfect" adherence (daily); (2) "moderate" adherence (4 doses/week); or (3) "low" adherence (2 doses/week). We obtained trough spot urine and plasma samples during a 6-week directly observed therapy period and a 4-week washout period. TFV concentrations were compared between adherence arms using 1-way analysis of variance.
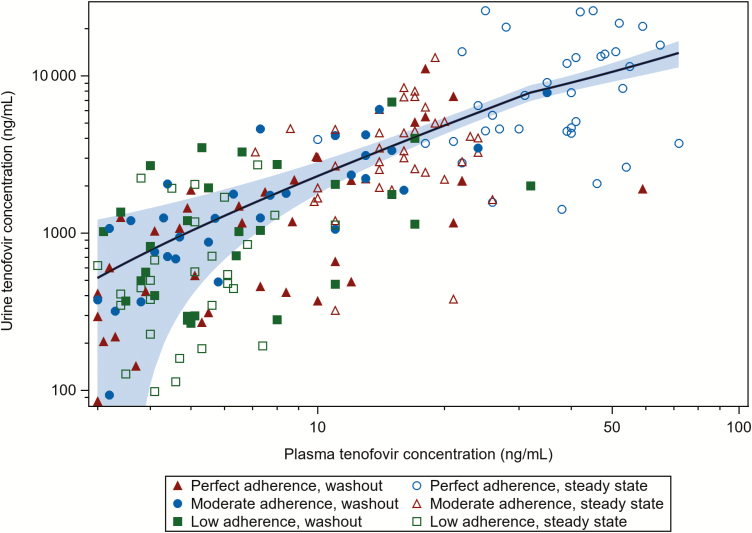
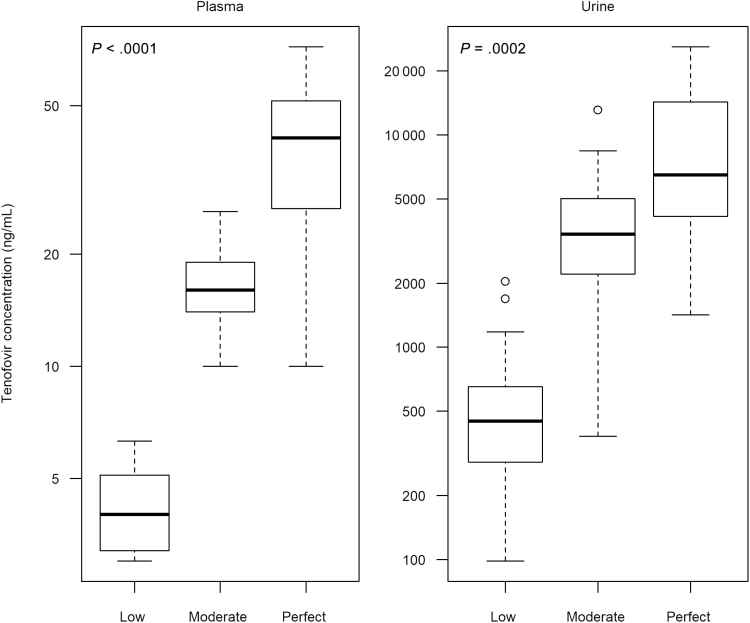
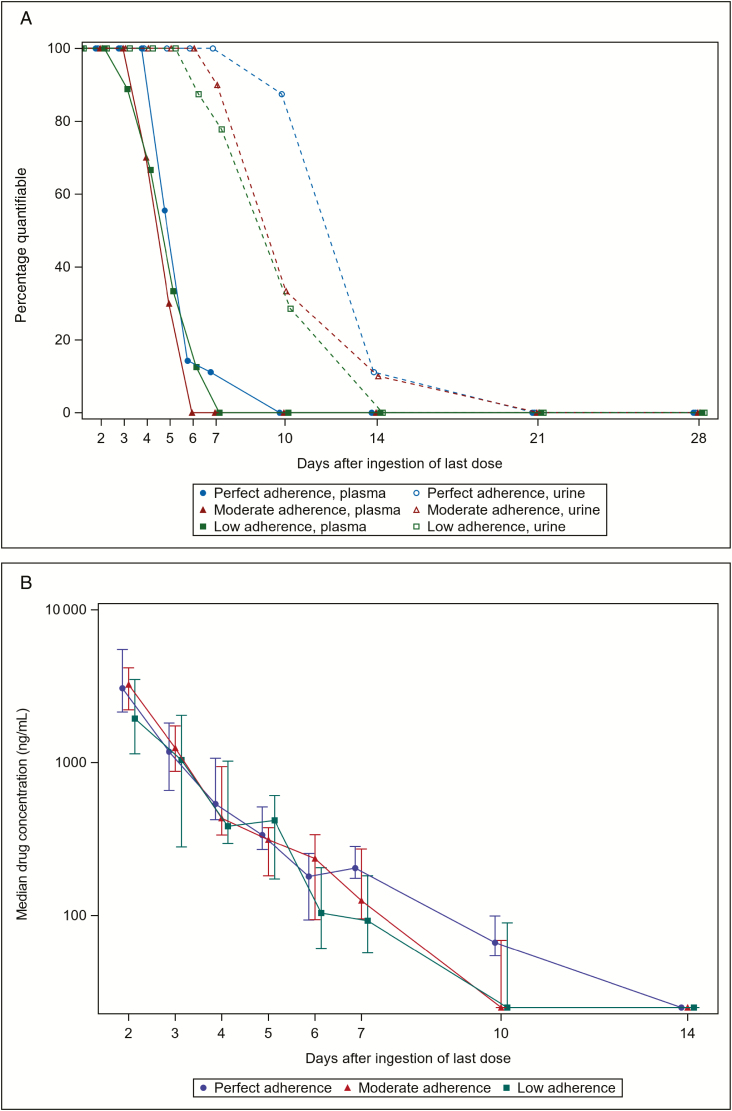
Results: Among 28 participants, the median age was 33 years and 16 (57%) were male. Correlation between TFV plasma and urine concentrations was strong (ρ = 0.78; P < .0001). Median (interquartile range) steady-state trough TFV concentrations (ng/mL) for perfect, moderate, and low TDF adherence were 41 (26-52), 16 (14-19), and 4 (3-5) in plasma; and 6480 (3940-14 300), 3405 (2210-5020), and 448 (228-675) in urine. Trough TFV concentrations at steady state were significantly different between the 3 adherence arms for plasma (P < .0001) and urine (P = .0002). Following drug cessation, TFV concentrations persisted longer in urine than plasma samples. Washout urine TFV concentrations and time to undetectable concentrations did not differ between the 3 randomized adherence groups.
Conclusions: Urine TFV concentrations can inform interpretation of novel point-of-care urine-based TFV assays to assess recent TDF adherence.
Clinical trials registration: NCT03012607
Trial registration: ClinicalTrials.gov NCT03012607 NCT03012607 NCT00301260.
Keywords: HIV; antiretroviral treatment; directly observed therapy; preexposure prophylaxis; tenofovir.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Adherence to Antiretroviral Therapy and Pre-exposure Prophylaxis: TARGETing the Ideal Measure.Clin Infect Dis. 2020 May 6;70(10):2152-2154. doi: 10.1093/cid/ciz651. Clin Infect Dis. 2020. PMID: 31314075 Free PMC article. No abstract available.
References
-
- Choopanya K, Martin M, Suntharasamai P, et al. Bangkok Tenofovir Study Group. Antiretroviral prophylaxis for HIV infection in injecting drug users in Bangkok, Thailand (the Bangkok Tenofovir Study): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2013; 381:2083–90. - PubMed
-
- Thigpen MC, Kebaabetswe PM, Paxton LA, et al. TDF2 Study Group. Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. N Engl J Med 2012; 367:423–34. - PubMed
-
- World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection 2016 Recommendations for a public health approach Available at: http://www.who.int/hiv/pub/arv/arv-2016/en/. Accessed 14 January 2017. - PubMed
