

Propofol Sedation Alters Perceptual and Cognitive Functions in Healthy Volunteers as Revealed by Functional Magnetic Resonance Imaging
- PMID: 31314747
- PMCID: PMC6640651
- DOI: 10.1097/ALN.0000000000002669
Propofol Sedation Alters Perceptual and Cognitive Functions in Healthy Volunteers as Revealed by Functional Magnetic Resonance Imaging
Abstract
Background: Elucidating networks underlying conscious perception is important to understanding the mechanisms of anesthesia and consciousness. Previous studies have observed changes associated with loss of consciousness primarily using resting paradigms. The authors focused on the effects of sedation on specific cognitive systems using task-based functional magnetic resonance imaging. The authors hypothesized deepening sedation would degrade semantic more than perceptual discrimination.
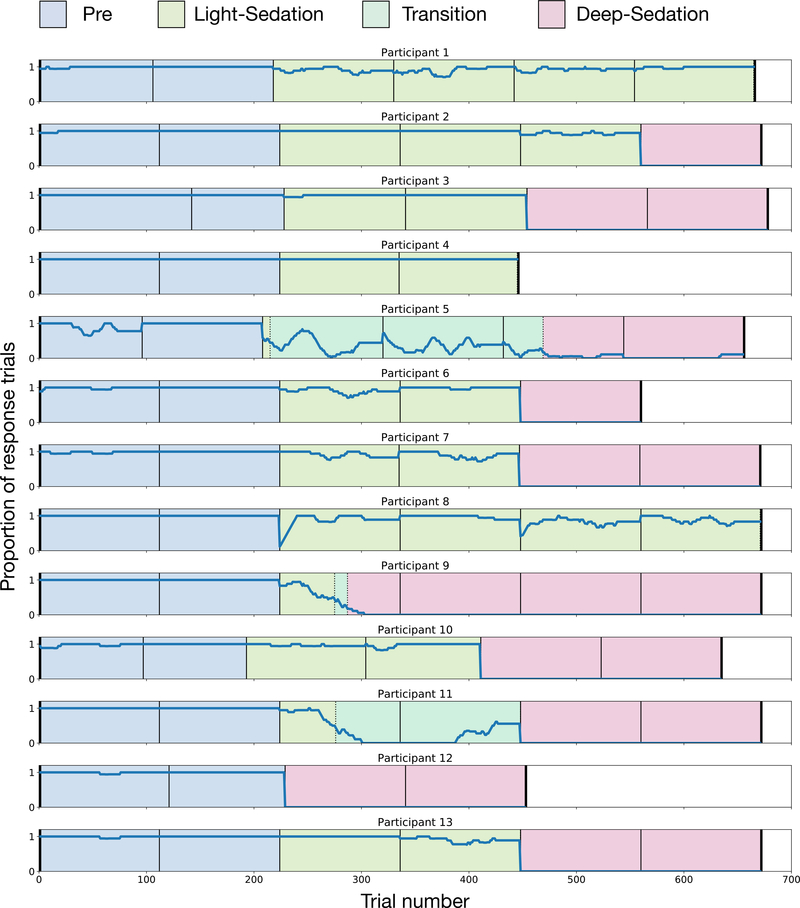
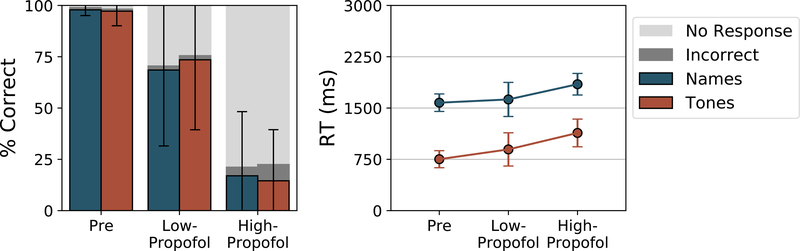
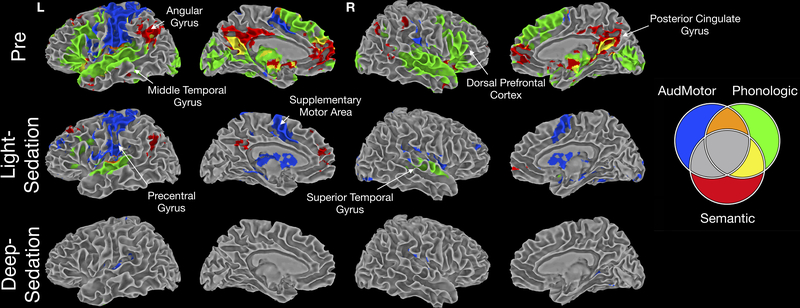
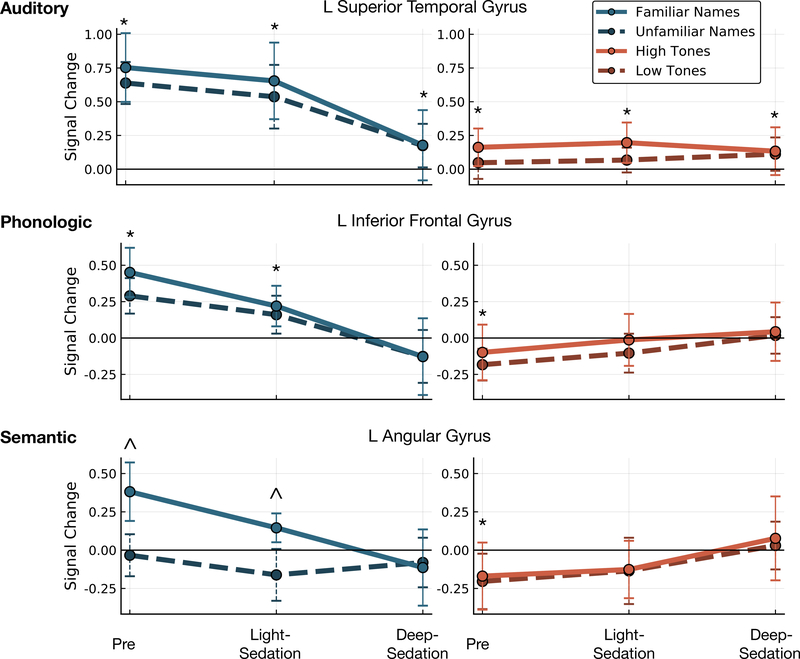
Methods: Discrimination of pure tones and familiar names were studied in 13 volunteers during wakefulness and propofol sedation targeted to light and deep sedation. Contrasts highlighted specific cognitive systems: auditory/motor (tones vs. fixation), phonology (unfamiliar names vs. tones), and semantics (familiar vs. unfamiliar names), and were performed across sedation conditions, followed by region of interest analysis on representative regions.
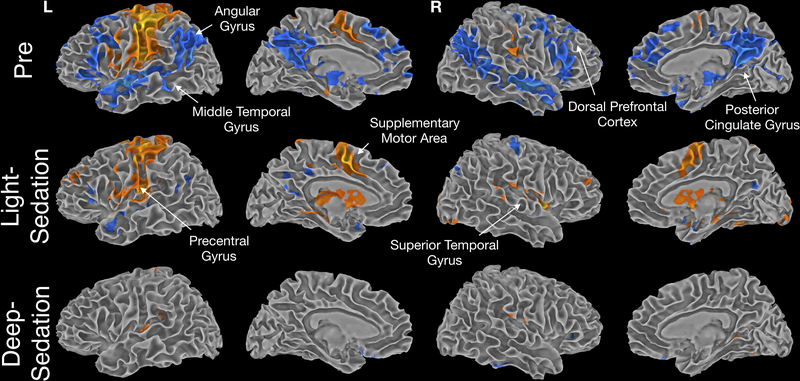
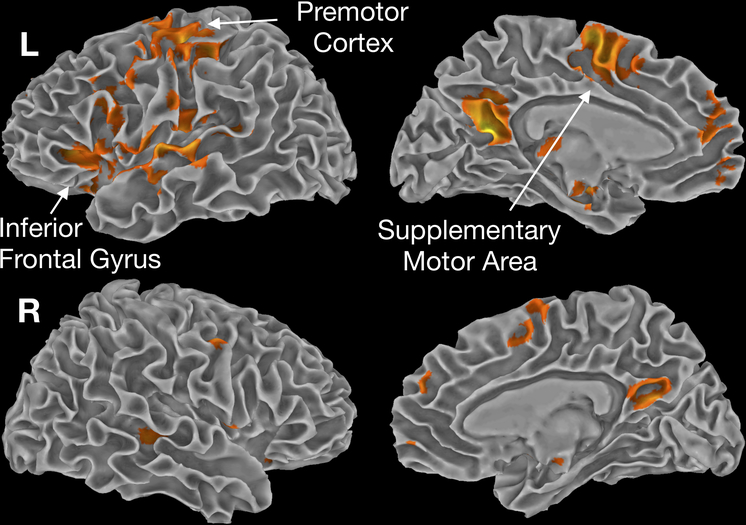
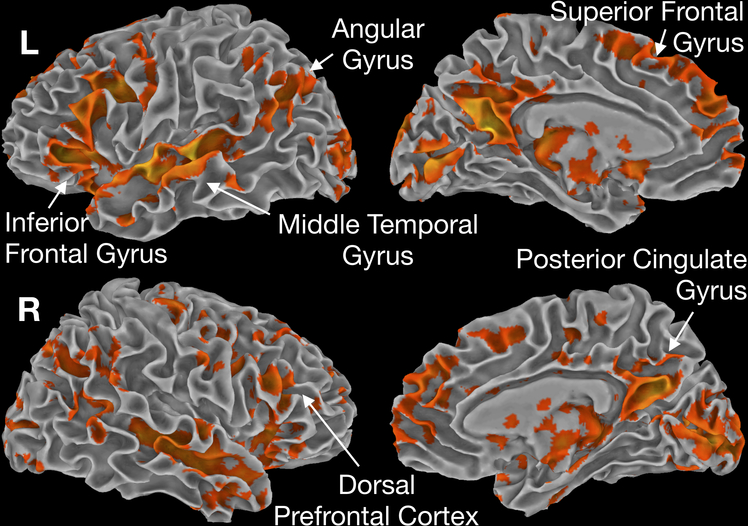
Results: During light sedation, the spatial extent of auditory/motor activation was similar, becoming restricted to the superior temporal gyrus during deep sedation. Region of interest analysis revealed significant activation in the superior temporal gyrus during light (t [17] = 9.71, P < 0.001) and deep sedation (t [19] = 3.73, P = 0.001). Spatial extent of the phonologic contrast decreased progressively with sedation, with significant activation in the inferior frontal gyrus maintained during light sedation (t [35] = 5.17, P < 0.001), which didn't meet criteria for significance in deep sedation (t [38] = 2.57, P = 0.014). The semantic contrast showed a similar pattern, with activation in the angular gyrus during light sedation (t [16] = 4.76, P = 0.002), which disappeared in deep sedation (t [18] = 0.35, P = 0.731).
Conclusions: Results illustrate broad impairment in cognitive cortex during sedation, with activation in primary sensory cortex beyond loss of consciousness. These results agree with clinical experience: a dose-dependent reduction of higher cognitive functions during light sedation, despite partial preservation of sensory processes through deep sedation.
Conflict of interest statement
Figures
Comment in
-
Non-Peer-reviewed Preprint Articles as References in Anesthesiology: Concerns.Anesthesiology. 2021 May 1;134(5):820. doi: 10.1097/ALN.0000000000003714. Anesthesiology. 2021. PMID: 33592106 No abstract available.
References
-
- White NS, Alkire MT: Impaired thalamocortical connectivity in humans during general-anesthetic-induced unconsciousness. NeuroImage 2003; 19:402–11 - PubMed
-
- Alkire MT, Haier RJ, Fallon JH: Toward a unified theory of narcosis: brain imaging evidence for a thalamocortical switch as the neurophysiologic basis of anesthetic-induced unconsciousness. Conscious Cogn 2000; 9:370–86 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
