

Effect of Universal Testing and Treatment on HIV Incidence - HPTN 071 (PopART)
- PMID: 31314965
- PMCID: PMC6587177
- DOI: 10.1056/NEJMoa1814556
Effect of Universal Testing and Treatment on HIV Incidence - HPTN 071 (PopART)
Abstract
Background: A universal testing and treatment strategy is a potential approach to reduce the incidence of human immunodeficiency virus (HIV) infection, yet previous trial results are inconsistent.
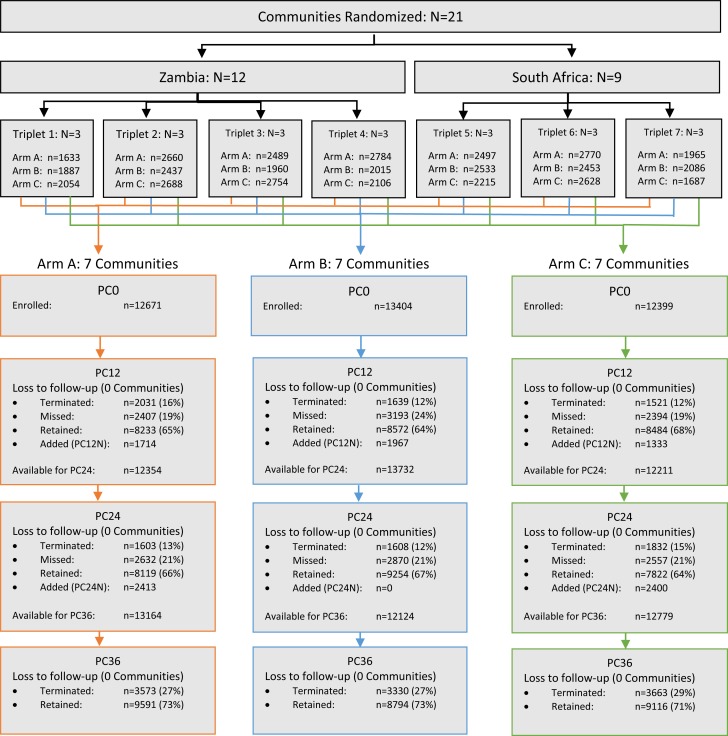
Methods: In the HPTN 071 (PopART) community-randomized trial conducted from 2013 through 2018, we randomly assigned 21 communities in Zambia and South Africa (total population, approximately 1 million) to group A (combination prevention intervention with universal antiretroviral therapy [ART]), group B (the prevention intervention with ART provided according to local guidelines [universal since 2016]), or group C (standard care). The prevention intervention included home-based HIV testing delivered by community workers, who also supported linkage to HIV care and ART adherence. The primary outcome, HIV incidence between months 12 and 36, was measured in a population cohort of approximately 2000 randomly sampled adults (18 to 44 years of age) per community. Viral suppression (<400 copies of HIV RNA per milliliter) was assessed in all HIV-positive participants at 24 months.
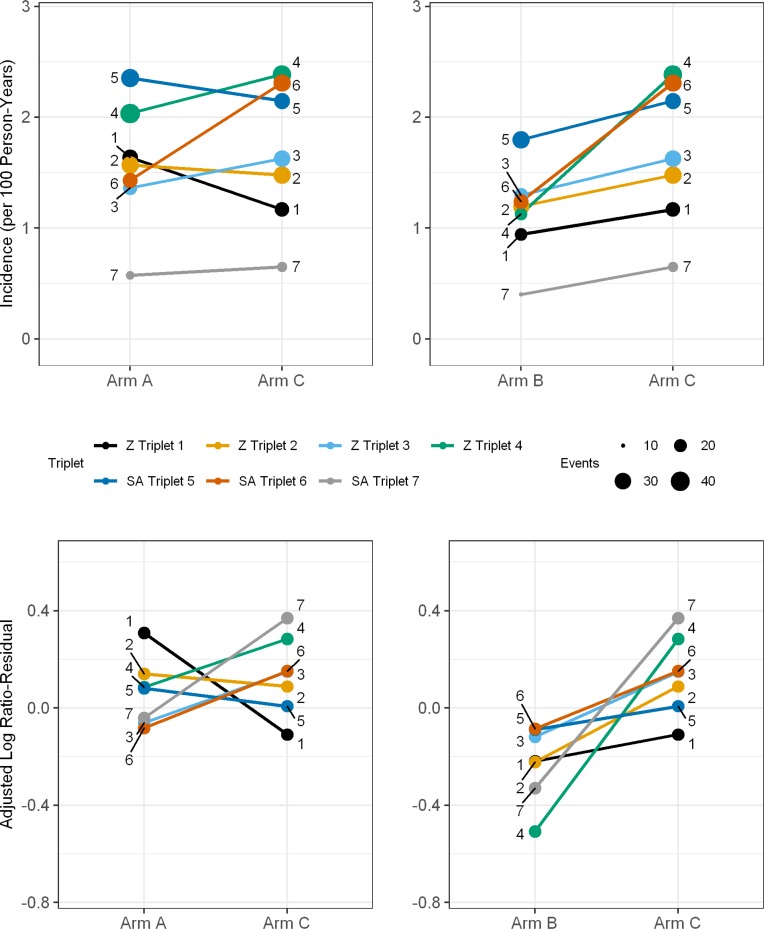
Results: The population cohort included 48,301 participants. Baseline HIV prevalence was 21% or 22% in each group. Between months 12 and 36, a total of 553 new HIV infections were observed during 39,702 person-years (1.4 per 100 person-years; women, 1.7; men, 0.8). The adjusted rate ratio for group A as compared with group C was 0.93 (95% confidence interval [CI], 0.74 to 1.18; P = 0.51) and for group B as compared with group C was 0.70 (95% CI, 0.55 to 0.88; P = 0.006). The percentage of HIV-positive participants with viral suppression at 24 months was 71.9% in group A, 67.5% in group B, and 60.2% in group C. The estimated percentage of HIV-positive adults in the community who were receiving ART at 36 months was 81% in group A and 80% in group B.
Conclusions: A combination prevention intervention with ART provided according to local guidelines resulted in a 30% lower incidence of HIV infection than standard care. The lack of effect with universal ART was unanticipated and not consistent with the data on viral suppression. In this trial setting, universal testing and treatment reduced the population-level incidence of HIV infection. (Funded by the National Institute of Allergy and Infectious Diseases and others; HPTN 071 [PopArt] ClinicalTrials.gov number, NCT01900977.).
Copyright © 2019 Massachusetts Medical Society.
Figures

Comment in
-
HIV-1 Epidemic Control - Insights from Test-and-Treat Trials.N Engl J Med. 2019 Jul 18;381(3):286-288. doi: 10.1056/NEJMe1907279. N Engl J Med. 2019. PMID: 31314975 No abstract available.
References
-
- UNAIDS Fact Sheet World AIDS Day. Accesssed 21st January 2019 2018.
-
- UNAIDS Miles to go—closing gaps, breaking barriers, righting injustices. http://wwwunaidsorg/sites/default/files/media_asset/miles-to-go_enpdf 2018;Accessed 21st January 2019.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical